Some of you may have become gently aware of a project that a small number of openEHR folks (mostly from vendors) have been quietly working on for the past few days. This came from an idea that @Bna of DIPS and his team had discussed of the need for some kind of app to help hospitals screen patients for risk of Covid-19.
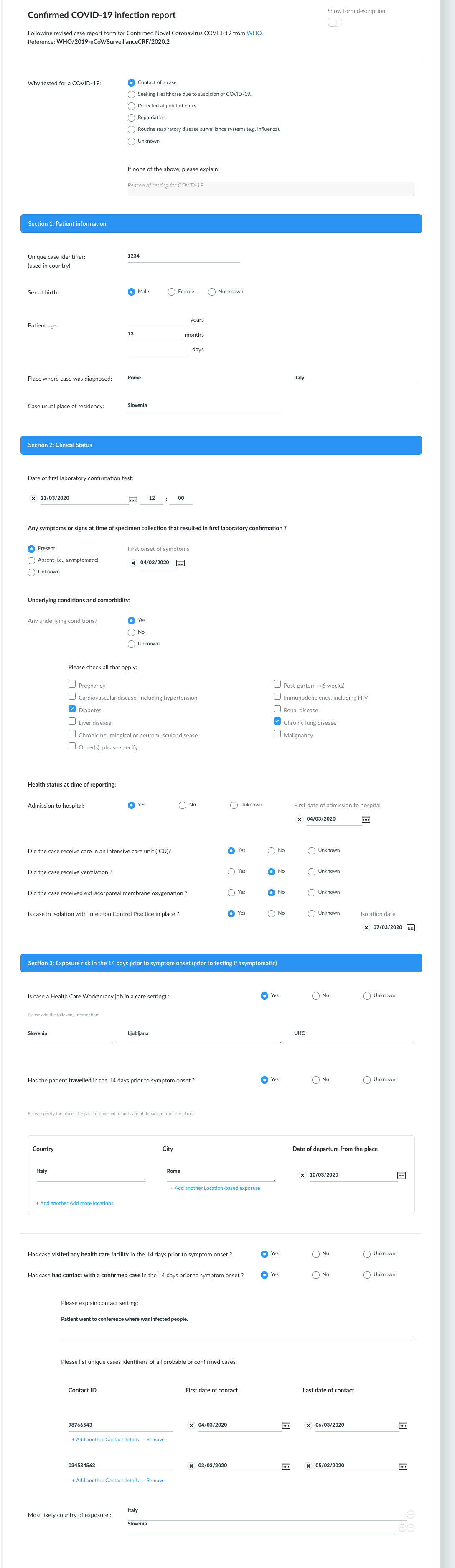
Basically this is the primary use case (good old fashioned paper form) from the US)
A citizen-facing equivalent has been produced by NHS-111 in the UK, using the Public Health England Risk assessment advice
Bjorn and I agreed that this seemed like an obvious need and definitely a role for shared template development but we wanted give ourselves some time to discuss with customers and public health experts as to whether such a screening app would give value, and to research the possible datasets that might be needed.
At the Rewired conference in London further discussions led to others coming on-board last Friday, particularly Better, with an expanded scope to also look at the WHO Covid-19 Reporting requirements
We were still anxious about going public until we had some practical experience and a much better handle on use of SNOMED-CT but invited a much wider group to a private Discourse topic, which we have now opened.
You will see what amounts to something of a brain dump but is testament to the willingness of this community to work collaboratively, sharing innovation and resource.
As of 10/03, 10 days after the very initial idea, and only 4 days (including 2 weekend days) after the majority of the work started we have achieved…
-
A Covid-19 screening assessment template has been created and uploaded CKM
-
A Covid-19 care report template has been uploaded to CKM, covering both the initial WHO report and outcome follow-up.
These templates are being used to underpin several apps …
-
DIPS have [a Screening assessment app] (Project Covfefe ) in live deployment at one site.
-
Better have a Screening assessment app in test at one site.
-
Better are developing a Case reporting app.
-
OpusVL are developing an open-source Screening assessment app
We have had huge support from other companies and openEHR members around offers to translate archetypes, help with decisions on correct SNOMED CT coding and general advice, with more companies and offers and suggestions emerging every day. We have had devs from different tooling vendors solve problems in minutes and analysts sharing their pathway diagrams and screen designs.
I am very proud to be part of a community which though small, through the strengths of some great technical underpinnings and specifications, the ongoing commitment and rigours methodology of the CKM clinical modellers and the devs in the various companies who make the magic happen, has shown just what we can do, and fast.
And we need to be fast because the screening questions and epidemiology changes daily - the apps and reports will change weekly.
So well done to all those who worked hard over a very small period to make solid start and to everyone else, please come help build on this work, which we are happy to make public with some sort of more formal announcement by openEHR International very soon.
We will continue the ongoing conversation in this topic…