Hi David - further thoughts from me!! Outcome of a long early morning walk!!
In current opnEHR terms, I think that is correct. The proper action for a corrected confirmed diagnosis, is probably to logically delete or update the original. Now there may be some benefit to setting the refuted flag before that update/delete.
But where refuted means ruling out a suspected diagnosis, the correct behaviour in current openEHR is to create a Specific Exclusion Entry, and not create a Problem/diagnosis at all.
The problem here is fundamentally that FHIR is carrying a message about the status of the Condition, but that does not necessarily map cleanly into how any target system handles negations/ exclusions/corrections etc. This is not unique to opnEHR, nor even to FHIR-native CDRs where how you handle ‘refuted’ may be very implementation-specific.
So there is simply no clean mapping solely at term-level or even structure that we can apply here in a universal way.
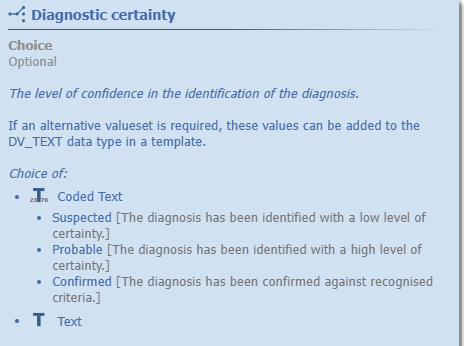
Preliminary –> Suspected
“Preliminary [The initial diagnosis made, usually associated with a low level of clinical certainty. It may change as test results or advice become available.
Established –> Confirmed
Refuted –> Refuted, where this is a correction to an ‘existing diagnosis’ (that may or may not have been confirmed!) and in openEHR, you have to decide what to do with the original diagnosis entry - update / delete/ flag. I don’tthink this can be done automatically
Refuted → as ‘Rule-out diagnosis’. Normally where a suspected diagnosis has been ruled out after investigation but no other accurate diagnosis is offered. e.g the Problem was a child with headache, rash and fever but is discharged with the diagnosis of ‘meningitis excluded’ , In openEHR cirrent advice is to import this as a Specific Exclusion.
@Lars - definitely not wanting to dodge the necessary semantic wrangles!! They are fun in their own way. Just cautioning against having agreement as necessarily solving the problem. We have to get into the expectation of what the recipient should understand and how to behave e.g should probable be rgarded as a working diagnosis from the pov of ongoing mgt/ AI / CDSS .
I think there is some value in setting the refuted flag in openEHR, but that should not be the only action - I think I would insist on any incoming FHIR ‘refuted’ conditions being queued for human review, if they are being imported into any kind of CDR where data quality and clinical safety is significant.
BTW I think the refuted term is probably in the wrong place. Currently it is on ‘Diagnostic status’ in the qualifier archetype. Diagnostic status was intended to capture the status of the diagnostic process leading to ‘Final diagnosis’ i.e all investigations exhausted vs Diagnostic certainty in the main archetype, which is about confidence in the diagnosis - you can have a Final diagnosis which remains unconfirmed. TBH this was probably over-engineered, but was an attempt to resolve where terms like final and working diagnosis fit. I donlt think refuted fits here but would do on Diagnostic certainty.
I’ll make a CR on CKM to see if it can be moved.
TBH I don’t think we have this ‘rule-out diagnosis’ issue sorted, either on the FHIR or on the openEHR side. Possibly something to chew over in the collaboration efforts. I am quite intrigued by the FHIR ‘Conditions excluded’ extension but I’ll post on that separately!!