As Public Health in the Netherlands we are learning lessons from the pandemic and are actively investigating if openEHR could be the foundation for the infectious disease control data model.
We invite you to a comprehensive discussion that delves into both the technical solutions and the semantic alignment of the Public Health Data Model within the OpenEHR Reference Model. Our focal point is finding answers to the question: “Does the Public Health Data Model semantically fit in the OpenEHR Reference Model?” while also exploring practical technical solutions.
Semantic Harmony: Share your insights on how well the Public Health Data Model aligns with the concepts and structures defined in the OpenEHR Reference Model. Where do you see alignment, and what challenges exist?
Mapping Strategies: Explore tools and methodologies that have been successful in mapping public health data elements to corresponding archetypes within the OpenEHR Reference Model. Are there emerging standards or best practices?
We encourage you to contribute both your technical solutions and perspectives on the semantic alignment of these models. Let’s collaborate on finding comprehensive answers to our overarching question while sharing technical solutions for the integration of the Public Health Data Model with the OpenEHR Reference Model.
Looking forward to a fruitful and insightful discussion!
FYI:
The central german corona data platfom was an openEHR CDR.
We also had a infection control use case in highmed (HiGHmed - Use Case Infection Control).
Slovenia also did some covid and openEHR related stuff (@johannes.schmidt maybe can shed some light into this).
We have another upcoming project where i will suggest a cooperation
Briefly, from previous experience:
The data relating to a person fits perfectly. The other data, properties of an ‘outbreak’, resources etc. doesn’t. It could be a AQL query. But saving the result would be a non openehr data model.
The SEC has talked about expanding the openehr reference model to include data not relating to a person. But this would require a strong leader with openehr experience.
There will be many advantages, mostly those from openehr in general (vendor neutral, scale of data, lifelong data, high quality models etc). But since outbreak management is often secondary usage of data that has been recorders in a primary EHR, it would significantly lower the admin burden on both reporters and GGD personnel, it would increase quality of data, it would decrease delay, etc. etc.
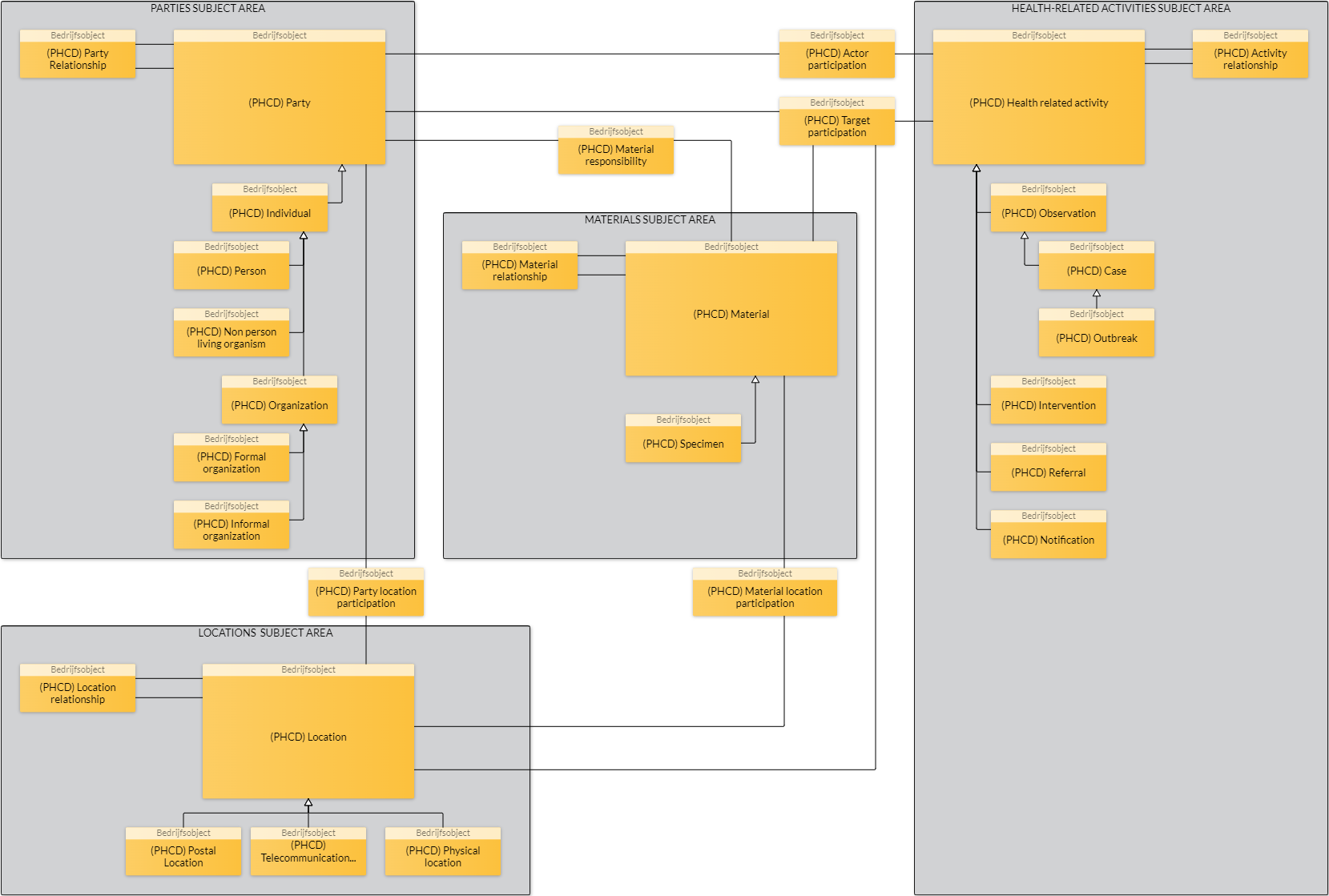
Health related activities definitely fit in the openEHR ‘EHR’ space
The ‘parties subject’ is largely covered by the openEHR Demographics model, but this has so far not been widely deployed/implementers, and as you say would need to be extended a little to support organism and outbreak as entities. For me, this area is less compelling to be done in openEHR ‘dual modelling’ as more traditional modelling/database approaches will handle this more easily than the complex clinical data.
As Joost says, it would need a bit of a deep dive below the high-level diagrams above to really understand if openEHR demographics offers a significant advantage, and therefore worth investment. For the clinical aspect, it is a no-brainer!
I’ve been working on a growing library of models to support national infectious disease surveillance by the MOHW Jamaica. There are early versions of some within CKM, now mostly outdated.
Later versions are local to my private repository but shared here. It is intended to upload them to CKM as draft candidates in the near future:
Hello Arne!
As for the health/clinical considerations and questions, I think the answers given are crystal clear.
As for the public or demographic aspect, I think your architectural picture already reflects the nature of the data very well! So why try to lump everything together?
You might find this article (which is also very general) useful:
I’ll try to dive a little deeper into the Slovenian approach next week.
Hello Arne,
as promised here is some more information i received from my colleagues.
The Slovenian Covid project had the advantage of being able to reuse the existing infrastrucure and data.
→ Vaccinations (also allergies, diseases,procedures,…) were already recorded via the “Slovenian national patient summary template”.
Only two new templates were introduced for the COVID use case (covid screening and sequencing). The main archtetypes were:
Regarding the public health data model you referenced:
Thank you for this source. Although quite old, it was an interesting read.
In fact, the subject area “health related activities” is perfectly suited for openEHR - including all the detailed considerations on relationships, data types and multiplicities. Most of this is already mapped in the international archetypes and ready to use!
I also see openEHR as a suitable technology for the subject area “materials”. However, suitable archetypes probably still need to be developed or existing ones extended. Models already exist for the specimen or food examples provided in the paper. “For other types of materials of interest to public health such as lakes, rivers, national parks, trains, planes, s, or ships, other coding systemswill be applicable”
Well, here I would refer to much more experienced and better modellers - looking forward to comments from @heather.leslie / @ian.mcnicoll. Maybe it is enough to capture these materials e.g. via an advanced version of Evaluation Archetype: Exposure [openEHR Clinical Knowledge Manager]?
As Ian has already written, we as implementers have not yet used the demographic model of openEHR and rely on FHIR here. The resources listed for individuals and entities are highly mature.