For a project about SNOMED CT coding of nursing diagnoses I’m creating a template with a set of diagnoses names with corresponding SNOMED codes. For each diagnosis name the user records, a corresponding SNOMED code should be persisted.
I’m aware of different ways of achieving this result. So I’m looking for an assesment of those options.
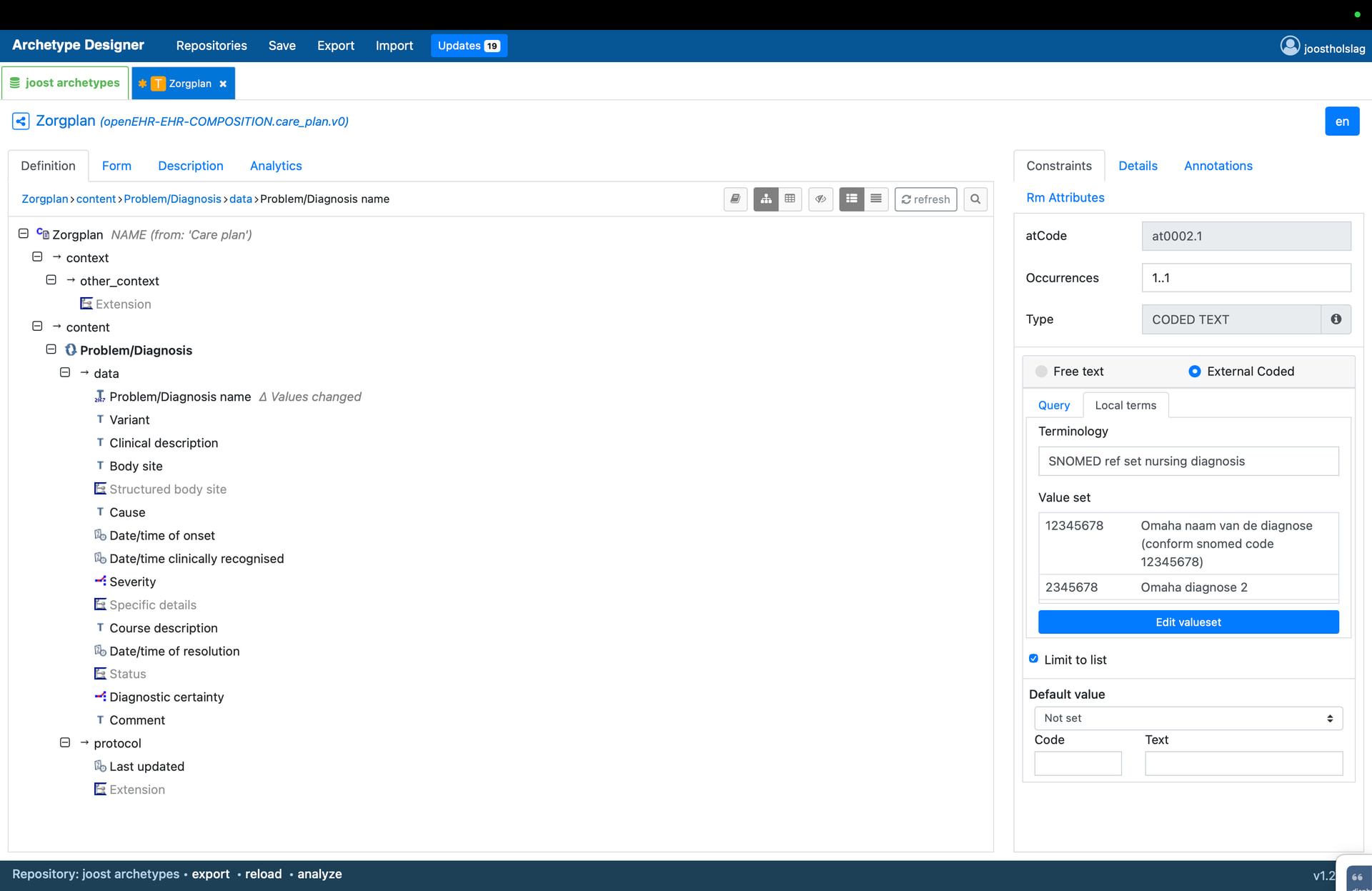
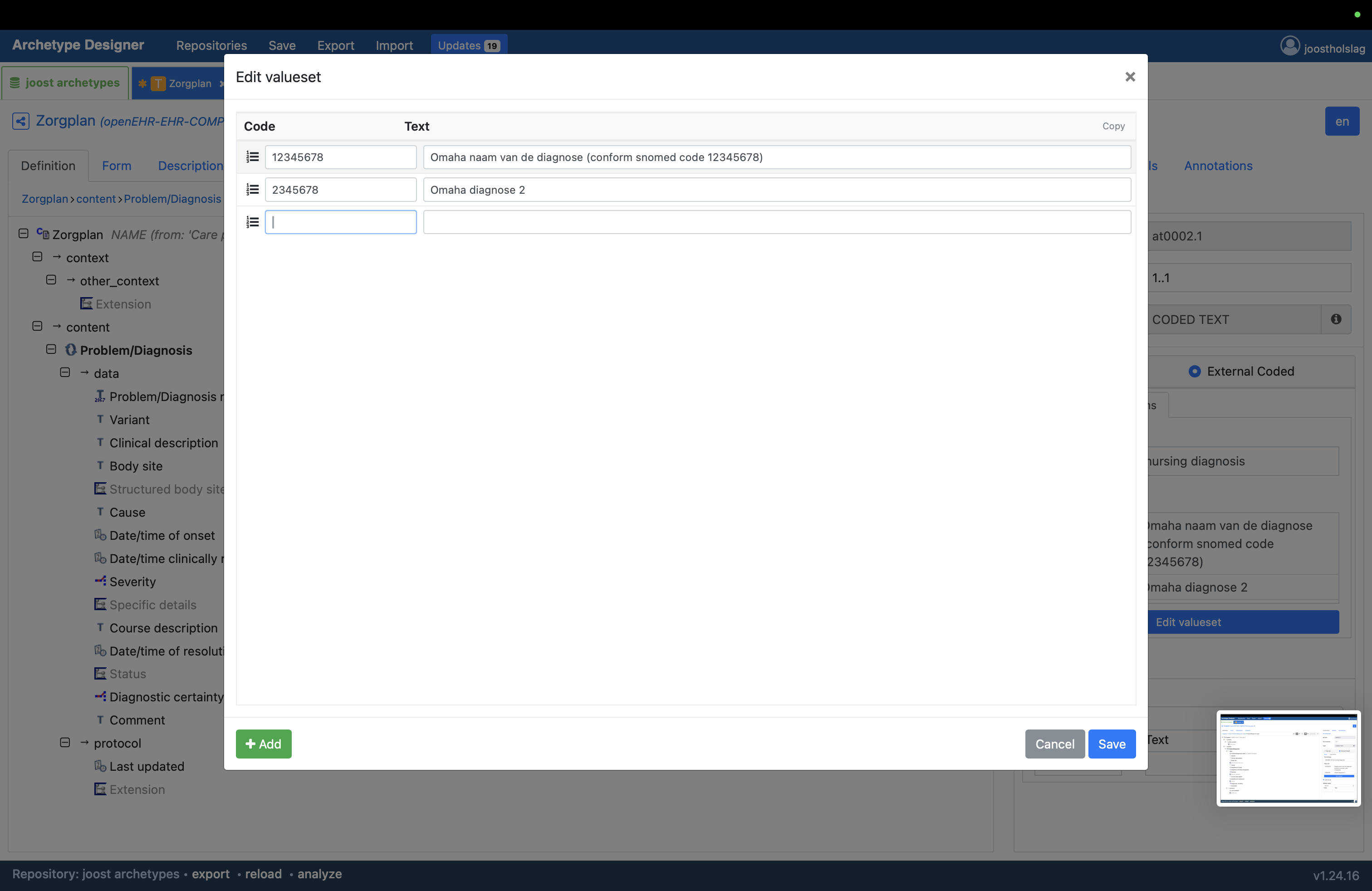
A common practice, I believe, is to, in the Template, set the SNOMED code as the ‘code’(_string) for a DV_CODED_TEXT, with the value as ‘text’, right? This lets you query on the DV_(CODED_)TEXT.code_string based on the snomed code.
However the Class description states this as misuse, right?
Misuse: If the intention is to represent a term code attached in some way to a fragment of plain text,
DV_CODED_TEXTshould not be used; instead use aDV_TEXTand aTERM_MAPPINGto aCODE_PHRASE.
In addition: this does not allow interaction with the user in selecting the appropriate SNOMED code. So it only works (clinically) safely if the match of DV_CODED_TEXT code and value are a 1:1 match. In my experience this is often the case, but also frequently not.
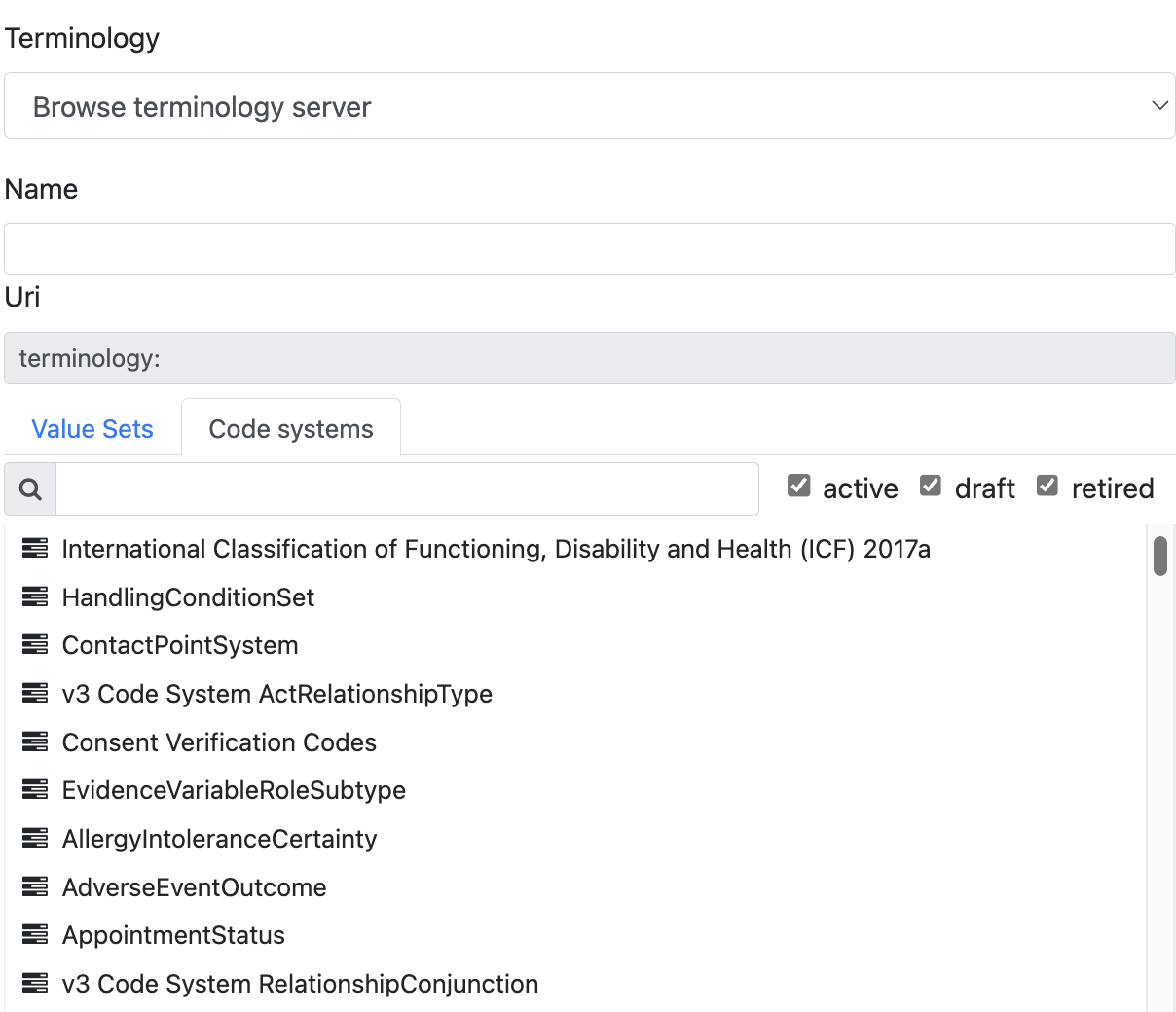
Now (at least in ADL2/AOM2) there’s a ‘term_binding’ in every archetype and template that allows binding of any local code (e.g. those in a DV_CODED_TEXT.defining_code) to a code in an external terminology e.g. SNOMED.

(CKM test showing an ADL2.4 rendering of term_bindings to SNOMED CT (for ELEMENT names, not values)
Now if that code needs to be persisted e.g. in order to query on it based on native SNOMED codes, that term_binding code ‘goes into’ DV(_CODED)_TEXT.TERM_MAPPING. It’s up to the client application to do that. And to interact with the user for confirmation or selection etc.
I think this is the safest pattern to use right now, but I’m unclear on the support for it in ADL1, tooling, and CDRs. But migration re archetypes/templates, persisted compositions, queries and apps seems high impact.
And finally I think we as openEHR are moving towards using FHIR value sets as the preferred way of expressing coding of values in a set. So it would be good to take that into account before changing modelling practice.
Right now I’m looking for verification of my analysis above. And for real world experience around (template) modelling and querying.