Here is a sample of simplified code working with blood pressure template:
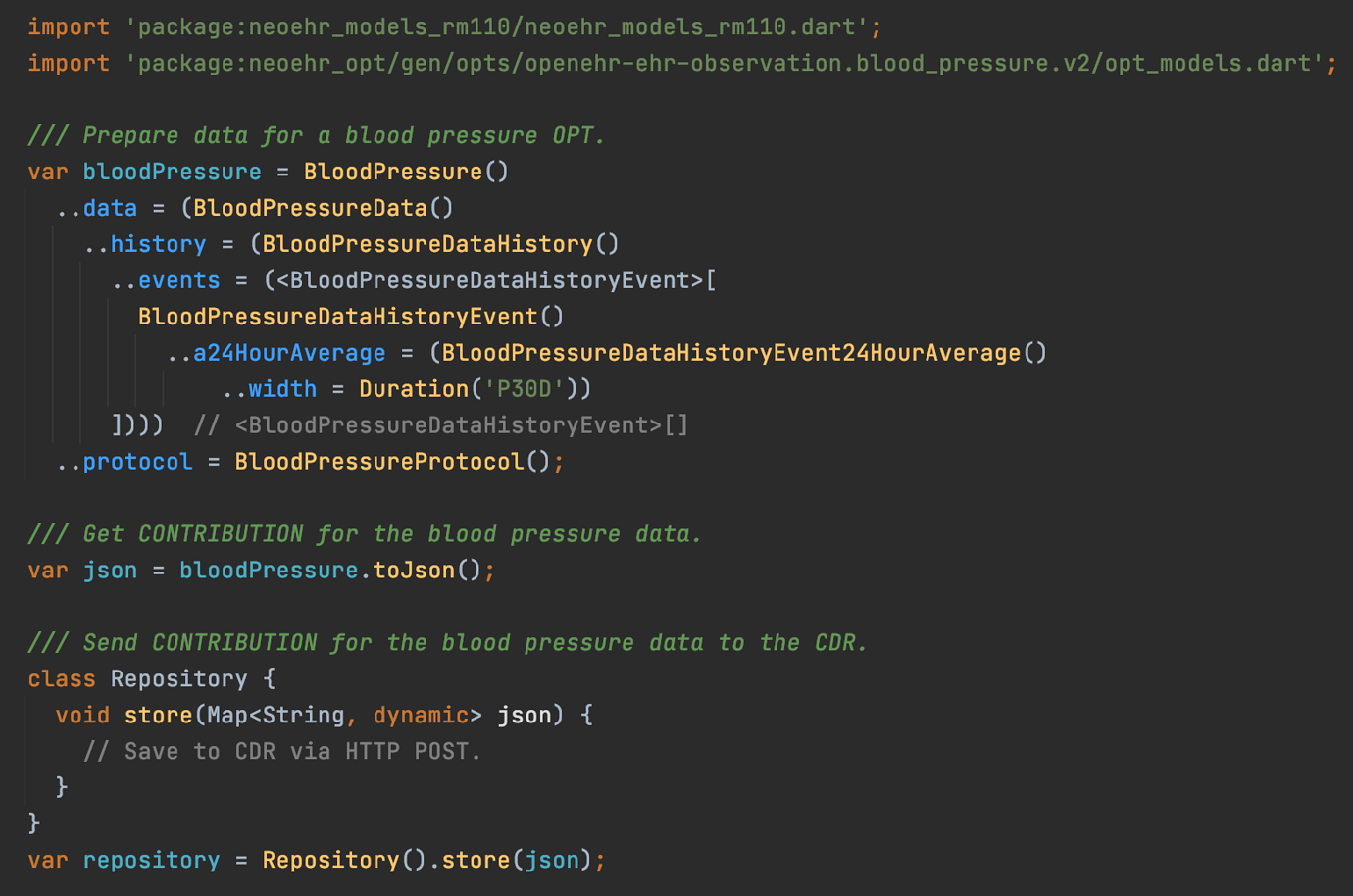
More in this answer.
More about the generator’s code in this answer. It takes only a few lines and the generator can output code in TypeScript, C#, Kotlin,…
Here is a sample of simplified code working with blood pressure template:
More in this answer.
More about the generator’s code in this answer. It takes only a few lines and the generator can output code in TypeScript, C#, Kotlin,…
| Topic | Replies | Views | Activity | |
|---|---|---|---|---|
| Link between goals and other clinical concepts | 43 | 2 | 27 June 2014 | |
| lessons from Intermountain Health, and starting work on openEHR 2.x | 30 | 3 | 8 October 2012 | |
| Choice between data element and SLOT? | 41 | 2077 | 8 March 2021 | |
| Data extraction from openEHR - a demanding and challenging task? | 25 | 632 | 19 August 2025 | |
| Compact XML format...? | 45 | 0 | 29 November 2007 | |
| openEHR archetypes as SQL Tables | 58 | 911 | 26 February 2026 | |
| What happens once the Pulse/Heart beat archetype is replaced? | 48 | 360 | 2 October 2025 | |
| EHRBase and ADL2.0 | 23 | 781 | 13 April 2024 | |
| openEHR API implementation in Rust | 44 | 1697 | 23 June 2023 | |
| TDS (and TDD) implementations? | 23 | 8 | 14 June 2013 |