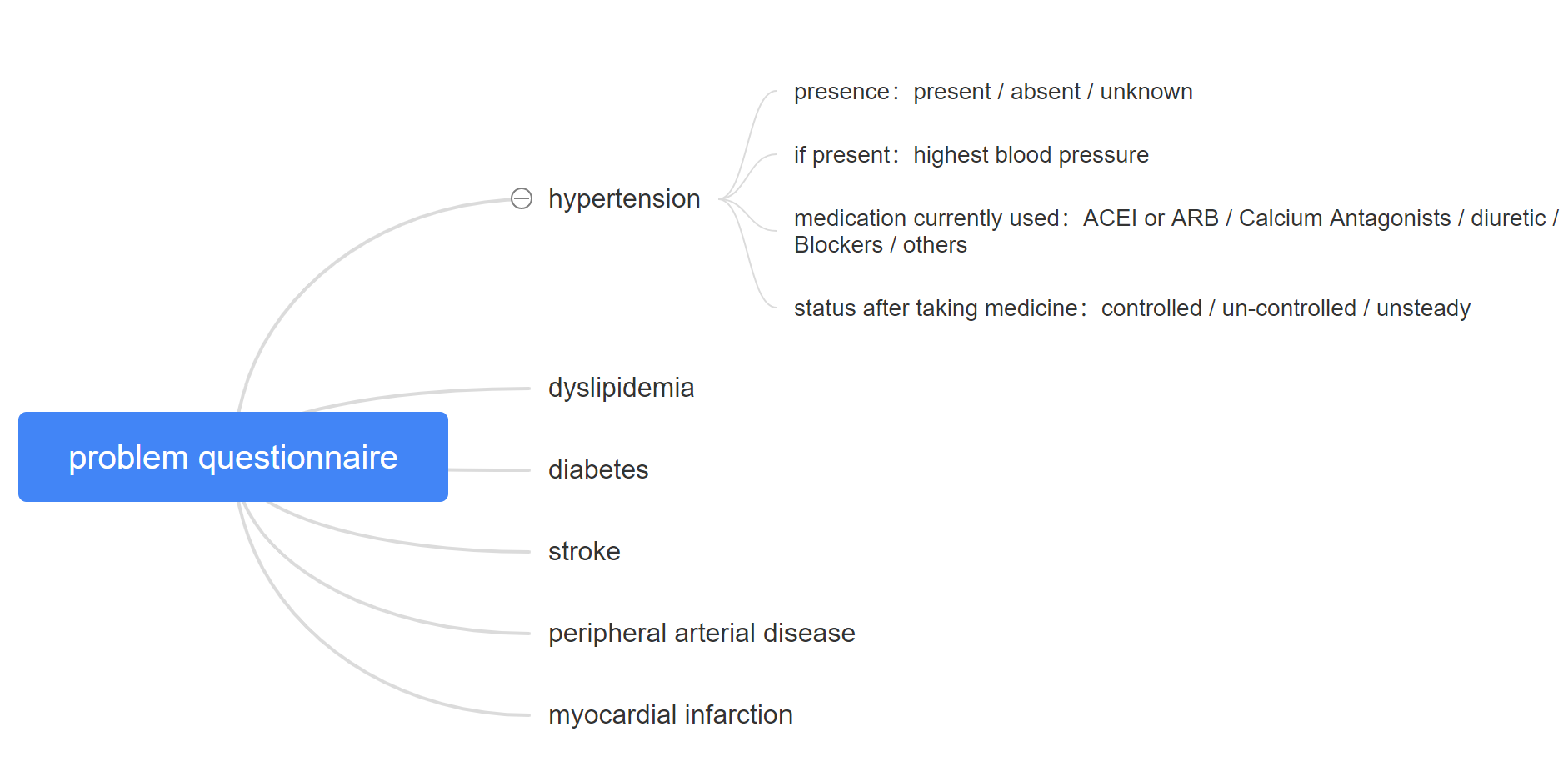
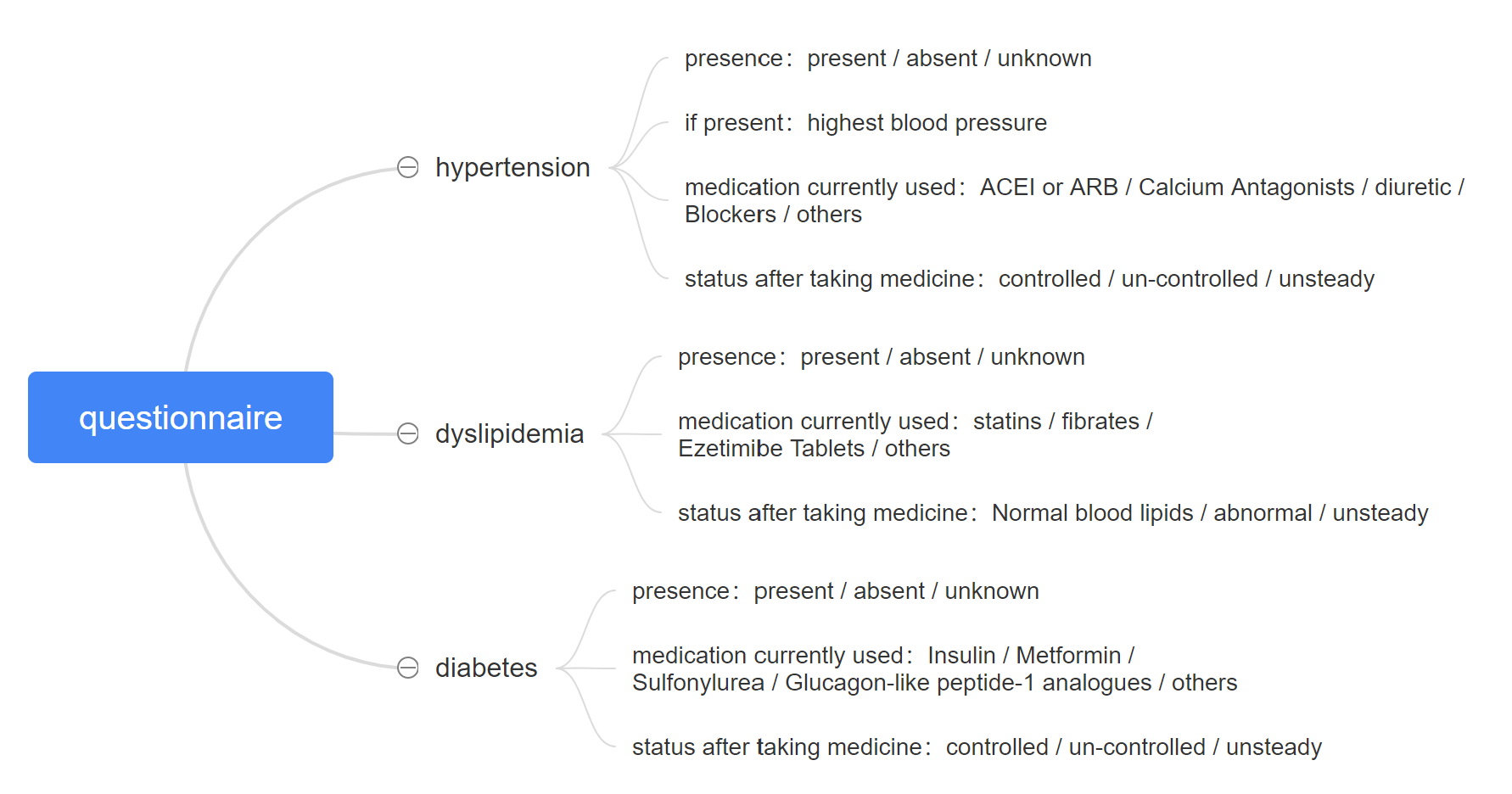
Is there any existing archetype to express the relationship above, if not, is it necessary to create a new archetype? I’ve tried Symptom/sign qustionnaire and Problem/diagnosis, but both cannot conclude medications. I think it is difficult to express the relationship between disease and its medication.
I would appreciate it very much if anyone can give me some advice~~
The presence of a “present/absent/unknown” leads me to think that we’re looking at a questionnaire. Since hypertension, diabetes, etc are problems, diagnoses or conditions, I would think the ‘Condition screening questionnaire’ (https://ckm.openehr.org/ckm/archetypes/1013.1.4442) would be your top level archetype. Further, the medications currently used could be expressed using the ‘Medication screening questionnaire’ archetype (https://ckm.openehr.org/ckm/archetypes/1013.1.4677). The highest blood pressure can be expressed using the blood pressure archetype, perhaps using an interval event with the mathematical function “maximum” if appropriate. I’m not sure exactly what is meant by “status after taking medicine”, so I’d need some more context to give advice about that.
These archetypes are all OBSERVATIONs, and can’t be nested within each other. However, the template could potentially provide the necessary context to bind the information together, the archetypes don’t necessarily need to be nested to show a relationship.
A screening questionnaire is a useful starting point, but that is all it is. For screening. We can’t possibly create a model that will cover all of the conditional statements that might evolve from that point. So we deliberately don’t model more info than this. Modelling data sets then relies on adding in the purpose agnostic archetypes in the same template to provide the recording/commit context - BP, Medication orders or ACTIONs to record any results of the ‘if, then’ logic. And let the clinical systems build the logic to work out when to offer additional screens etc.
I will have a go at interpreting the ‘status after taking medicine’ - meaning that after X days or weeks, the blood pressure is taken and recorded again. If the systolic/diastolic/either/both are higher/lower than the baseline recording then record an assessment of ‘controlled/uncontrolled/unsteady’, probably using the ‘Clinical interpretation’ data element in the Blood Pressure archetype. Does that come close? It contains so many assumptions that need to be clarified or recorded. We have the archetype structure but the business logic within the clinical system needs to drive what appears to be a simple statement about ‘status after taking medicine’. It is not simple, and there are so many variables, all of which need to be defined prior or recorded contemporaneously to enable the data recorded to make sense.
Thanks for the advices! Very helpful and clear up my doubt about the questionnaire archetype.
Dr. Heather’s interpretation for the confusing ‘status after taking medicine’ is very close to what it means which also reminds me that many terms in this template are actually not defined clearly. I should get down to solving this problem first.
I checked these archetypes and yes they indeed meet my needs, and the maximun event is a good idea, I should give it try! Thank you!
I’ve thought about this some more, and it seems to me like this is intended to be a statement about the diagnosis of ‘hypertension’, and not about a specific blood pressure measurement (or even an average or maximum BP over an interval of time)?
Good point. Depends on the intent of the data point. Is it the status after taking one dose eg urgent med to drop dangerously high BP or the diagnosis, which is long term?
These elements are in fact specially designed for recording the past history of a potential patient suffering from coronary artery diseases. The maximum BP is an oberservation, but the duration is not explicitly defined, it refers to the maximum BP in his/her BP history.
I found that Medication screening questionnaire (https://ckm.openehr.org/ckm/archetypes/1013.1.4677) is designed for one medication class instead of many classes, however in this case we have many 4 medication classes for Hypertension, 3 medication classes for Dyslipidemia and 4 for Diabetes. One way to express them is to clone 11 Mediacation screening questionnaire archetypes and only use its medication class cluster. Another solution is to extend this archetype which I think may distort its original meaning?
You can’t put mathematical function against a point event. The maths function basically means “this is the maximum measurement taken during this interval of time”, which doesn’t make sense for a point in time only. However, you could create an interval event covering the time from the person’s time of birth until the time of recording.
We’re suggesting using one instance of Medication screening questionnaire and creating 11 instances of the Medication class cluster. Would that work for your purpose?
I’m going to suggest taking a step back and ask @shiley about the context of the question…
Who is asking the questions?
Who is giving the answers?
What is the information used for?
Is the information collected regarded as being the definitive truth in the patient record. i.e if I say that hypertension = present does this have the force of actualling recording that as a diagnosis, or (as I suspect) is this really about someone reviewing existing records and summarising it / checking for particularly important information e.g. the highest recorded blood pressure - of course that information may not exist in electronic form.
Does anything recorded here trigger any kind of decision support?
Knowing more about the context of use makes it easier to advise.
We’ve thought about it but the class cluster is not repeatable (https://ckm.openehr.org/ckm/archetypes/1013.1.4677), that’s why we are thinking of extend this archetype by making the class cluster a repeating cluster. But as I mentioned above, I am afraid it may distort its original meaning.
This is a form designed by a group of doctors, and the answer is given by patient and recorded by nurse. We collect these basic information from patient who is going to have a CCTA(Coronary CT Angiography) test. The controlled status means ‘SBP<140mmHg and DBP<90mmHg’. But I have to admit the form doesn’t define everything clearly and cause some problems during modelling.
Ahem .
The intent of the ‘Medication class’ cluster was intended to be 0…*
I have now corrected it and uploaded a revised version to CKM.
Thanks. Good pick up!
Thanks for all~~ We’ve solved the problem based on the advices!!!
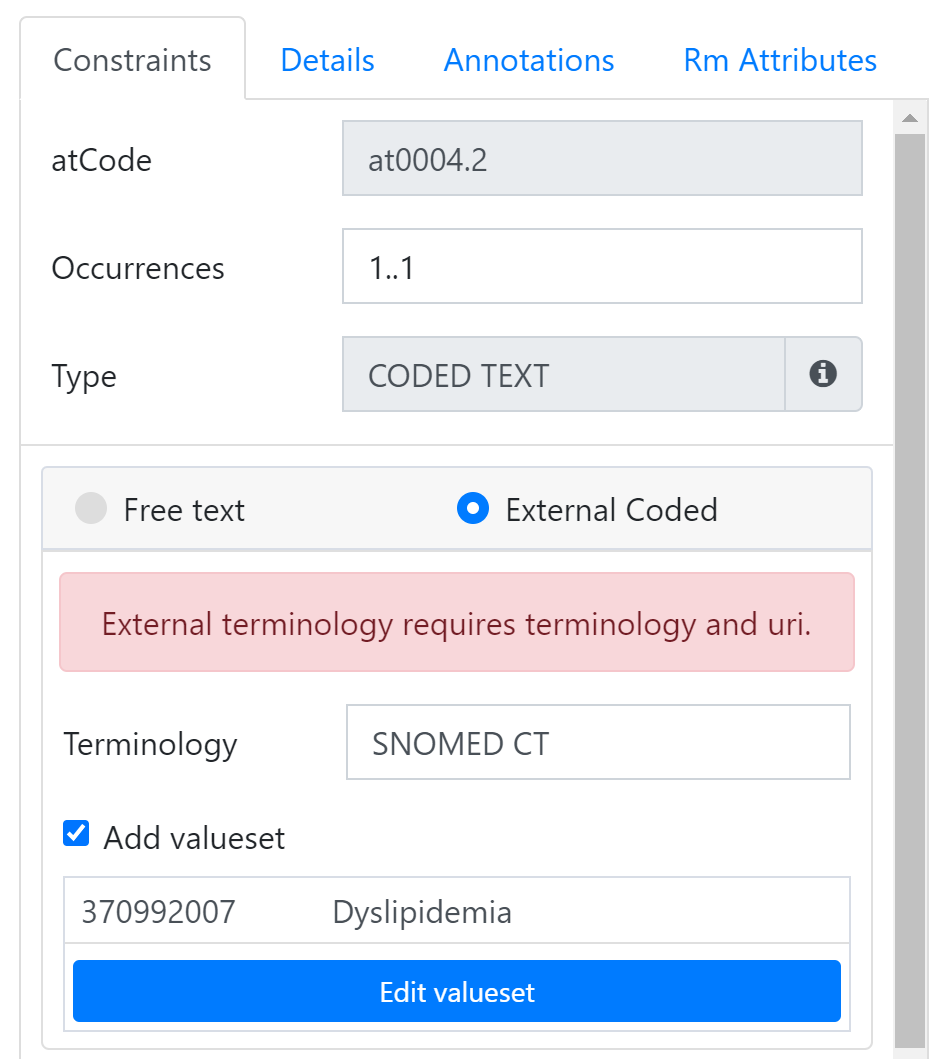
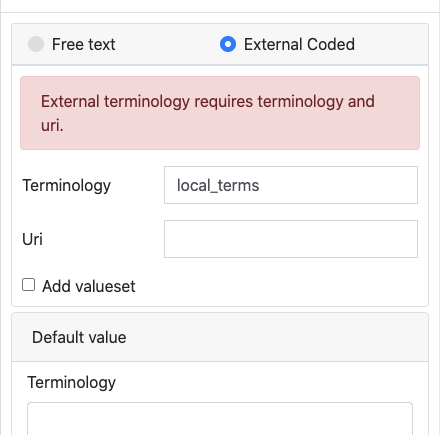
Also, I am confused about how to bind terminology in ‘Archetype Designer’ (https://tools.openehr.org/designer/#/). To be exact, I am trying to edit valueset when I am modelling a template, but ‘External terminology requires terminology and uri’, I am not sure what is ‘URI’ because whatever I put in, it would’t work…
I am so sorry to reply you this late!!! And thank you very much for the detail explanation! I was trying to bind terminology with SNOMED CT, and now I think I just need to hook up my template to SNOMED CT’s external terminology service as you instructed!
Sorry again for my bad memory! It seems multimasking will consume one’s memory time for me to focus on one thing at a time~~
Oh I know the feeling!! You might not be able to hook the external server up ‘live’ right now as I think currently only supports their internal terminology service. However I understand that this going to change - CKM will support FHIR Valuesets soon, and I suspect Better may go down the same road.



 .
. We’ve solved the problem based on the advices!!!
We’ve solved the problem based on the advices!!! 
 time for me to focus on one thing at a time~~
time for me to focus on one thing at a time~~