Hey everyone,
we are performing a clinical study (pneumological use case) for which the following problems should be recorded by a clinician in a simple Yes/No fashion:
coughing, coughing up sputum, dyspnea, chest tightness, cyanosis, peripheral edema, lung hyperinflation, barrel chest, chest wall retraction.
First, I grouped these in the following two groups:
A, symptom-based: coughing, coughing up sputum, dyspnea, chest tightness
B, inspection-based: cyanosis, peripheral edema, lung hyperinflation, barrel chest, chest wall retraction
I´m currently using symptom_sign_screening.v1 for A and problem_screening.v1 for B, e.g. like this:
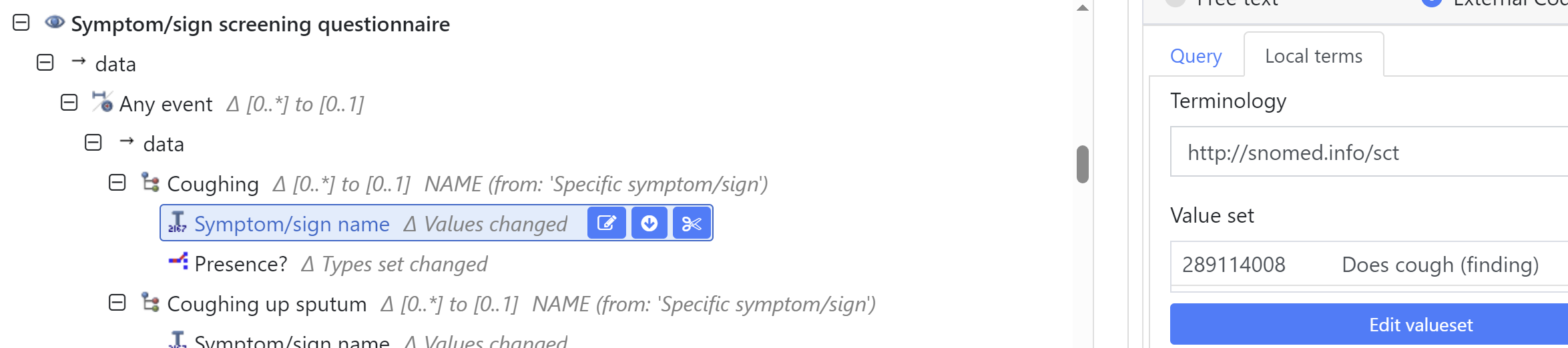
where I use a SNOMED Code for the symptom/sign name and Yes/No via “Presence?”
I have several questions to this:
- Can these screening archetypes generally be used in that way (for clinicians) or are they intended to be answered by patients only?
- Regarding the simple Yes/No answer, are these archetypes the right choice or would it be better to use problem_diagnosis.v1 and exclusion_specific.v1?
- when using SNOMED Codes as shown above, is it a problem to mix findings, e.g. 3415004 Cyanosis (finding), with disorders, e.g. 24228002 Barrel chest (disorder), in different clusters of the same archetype?
My understanding is that a finding is the result of an examination, however here we are not recording the examination itself.
This also makes me re-think which of the above mentioned problems is really just a symptom and what is already a diagnosis. In our study, the patients have the primary diagnosis of asthma or COPD, which is recorded elsewhere. Here we just want to know if they have these additional problems or not.
Thanks for your comments!
Kind regards,
Max