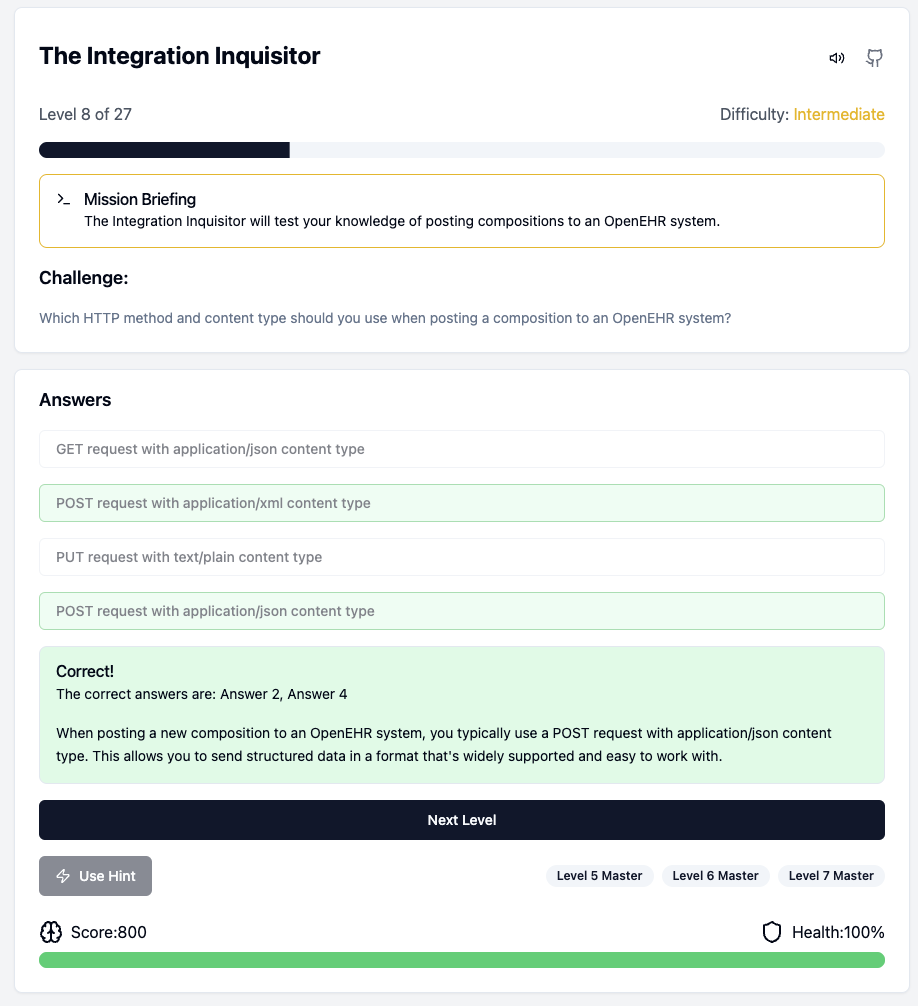
Gordon Mickel just posted an interesting, fun and interactive quiz game to learn openEHR concepts. Test your knowledge, earn badges, and become an OpenEHR integration master!
I was surprised about that one. In general openEHR CKM has a maximal modelling strategy. At this level this question is confusing to me.
I also don’t remember the message from @heather.leslie in Arnhem. And reviewing her ppt didn’t help.
I’m curious for some elaboration.
The way i understood the question is that: the aim of the archetype is always to get the max dataset but in specific cases such as the case of smoking, you have to divide it in different archetypes - you can have an archetype for consumption summary other for use, etc. But if theres a better explanation or if i understood it wrong, its always possible to open a issue in github and ask for clarification. I remember seeing a similar pattern in the alcohol case.
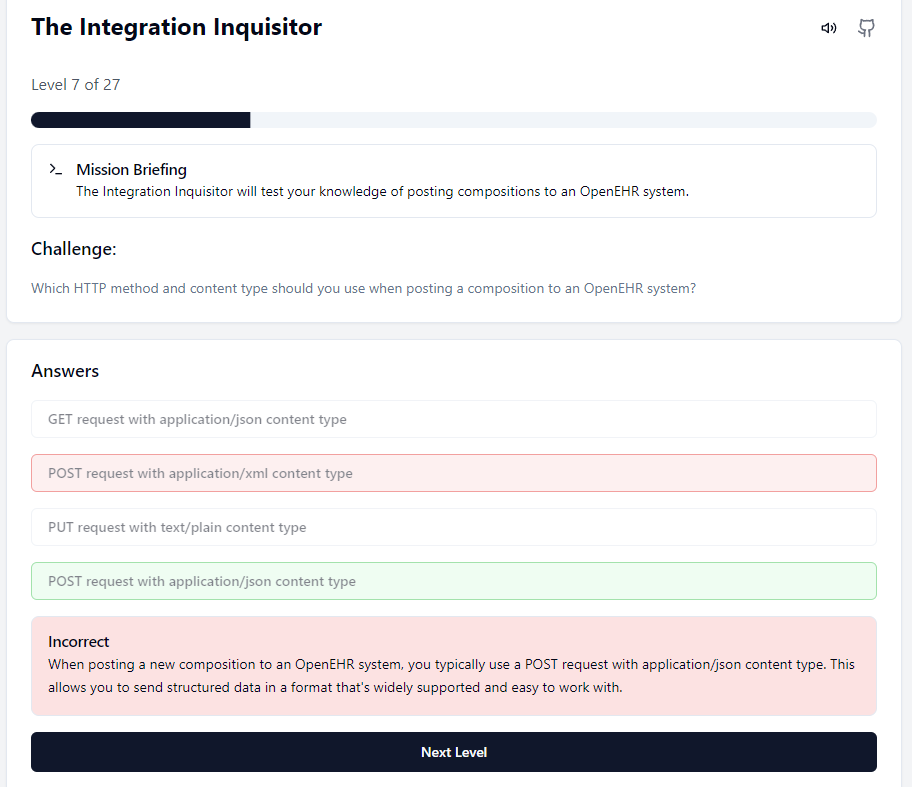
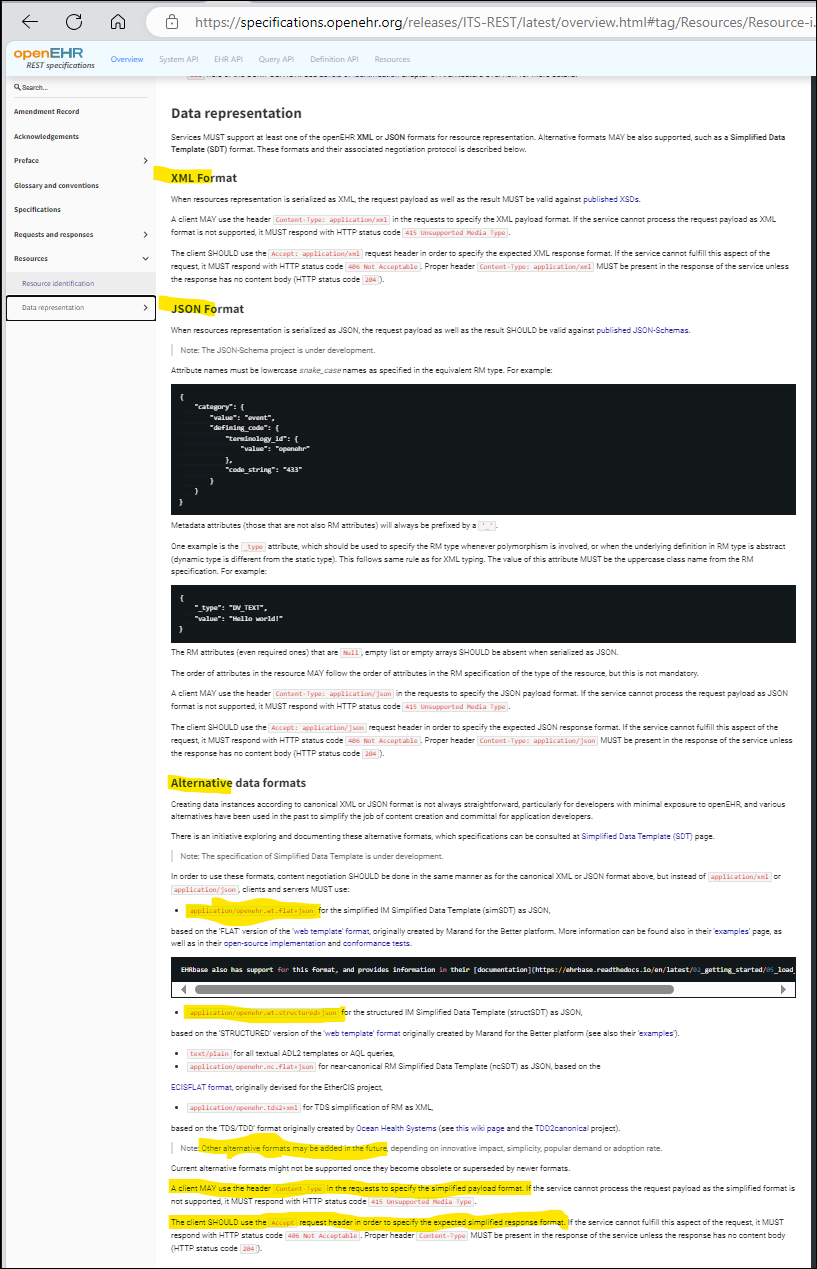
The quiz should be updated to not exclude any of the allowed representation formats (or to not list XML in the multiple choise). Read the full chapter under “Data representation” in Overview openEHR specs
We sometimes find the canonical XML format to be at least as useful as the canonical JSON format for some integration use cases, especially when the source system or some transforming part uses XML and you want to have e.g. an XQuery based transformation. Ask the Veratech people for example, right @yampeku & Co?
I want to start by thanking @borut.jures for sharing this quiz and @vanessap for the valuable feedback. It’s great to see it being used here!
A bit of background: I originally created this quick quiz for my co-workers before giving a presentation on OpenEHR for developers. It’s wonderful to see it reaching a wider audience.
Regarding question 7, you’re absolutely right. I’ll be working on allowing multiple answers to make it more accurate.
Well, you don’t have to, but trying to cram too much stuff into a single archetype will create a lot of avoidable headaches for both modellers, implementers and information consumers.
I for one agree completely with the answer given in the quiz: We asymptotically approach a maximal data set for each concept. But all aspects of smoking spans several distinct concepts.
I don’t use the word ‘maximal’ any more to describe what we do, rather aiming for ‘inclusive’.
Further complicated by the approach to achieving ‘inclusive’ is not always as simple as being limited to only one archetype per concept.
And of course, the final solution requires consideration on how to best represent the whole concept within a reusable ecosystem of archetypes.
Time for a new blog post Heather? I think the question of how to ‘select’ data elements for an archetype is very relevant. Given the FHIR 80/20 rule and the increasing collab. I’ve always liked the simplicity of ‘maximal’ to me defined as ‘anything some clinician wants to record about a specific concept’. But I now see that’s simplistic. At Nictiz the idea came up to make a ‘mind map’ (but less hierarchical) of all clinical data elements and their relations and selecting an area of related elements for a specific concept. They called it ‘betekenismodel’ (~semantics model). I hated the idea because it was very loosely defined yet made into a silver bullet. And because it’ll never be finished and you have nowhere to start doing implementable work. But given your and Silje’s described experience it may be more helpful then I thought. What do you think?
(Maybe let’s split this in a new topic)
I use the term “inclusive” to challenge the misconception that achieving 100% representation is not feasible or not necessary; rather it is setting the expectation that stakeholders who identify reasonable and semantically sensible requirements should be able to have them represented. Conversely, we don’t set a nominal target like an 80/20 split, since determining when 80% is achieved is equally as challenging and unrealistic as deciding when we have reached, or will we ever reach, 100%.
The ideal is that a published archetype to be approaching what we consider (sometimes guess) to be 100%, but circumstances and resource limitations often complicate achieving this. Each published archetype in CKM, no matter how rudimentary, is only published when it is clear what the plan is or pattern it will align with, drawing on past experiences and similar modelling patterns, and grounded by the rigor of the archetype ontology. It is not necessarily well documented at the moment, but if the way forward is not clear for a new archetype or archetype pattern it will be set aside until we can identify a viable path forward. This approach isn’t foolproof, but it is pragmatic and has so far served us well.
I’m not sure I understand what you mean by ‘betekenismodel’. But keen to understand more. Sounds like a new thread will be useful.