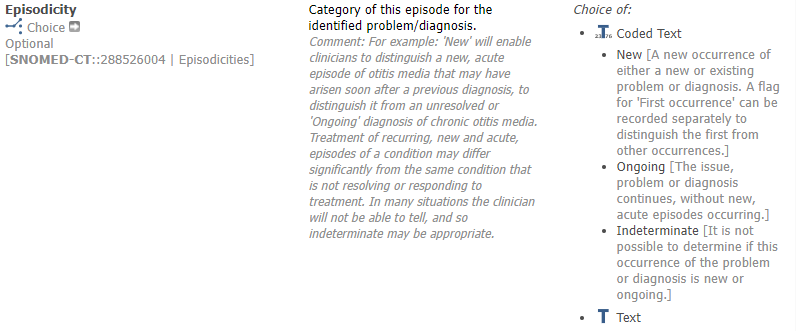
In a use case related to cancer, it is a request to classify the cancer condition within the three values:
New cancer
Relapse
Secondary cancer
There are various elements in both Problem/Diagnose and Problem/Diagnosis qualifier, but none does quite fit the value set. I do not want to split into several elements, so which one to chose?
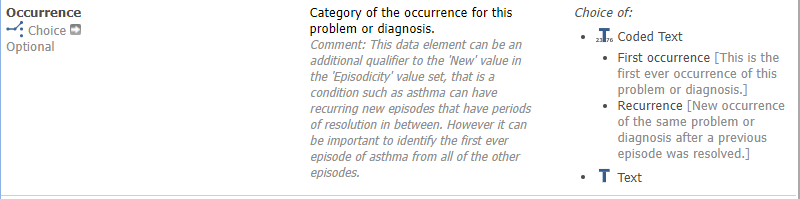
Problem/Diagnosis qualifier has two possible elements, maybe combined:
If you don’t want to split the elements, I think you are probably going to have to use a custom Cancer episodicity cluster.
We always recognised that it was going to be very difficult to get these problem-diagnosis qualifiers agreed as there are very often different approaches for different conditions, reporting requirements etc.
The semantics are important not to munge but teasing it out is often quite complicated.
New or relapse labels relate to episodicity.
A secondary cancer relates to extension/spread of the original/ongoing cancer
So, by my reckoning ‘secondary’ warrants a different semantic axis to new or relapse yet, in reality, all 3 are probably commonly grouped together in local registries.
If you can influence the data design, it may be worth exploring how to separate these concepts out.
If not, this is the reason why we have templates and even local non-interoperable archetypes.
Although if everyone expresses the munge in the same way, then we have to consider the politics of perpetuating the munge in a pragmatic template vs pushing back.
Over and out.
OK, the head of the actual cancer ward says:
“With secondary primary cancer”, we mean a new instance of cancer, not metastatic but with the same cause. Example: Heavy smoker, first having cancer in throat, cured. And later cancer in lungs. So not relapsed either. This will be a kind of “new episode” in episodicity, right?
Hmm… not sure . Episodicity is really trying to capture a new episode of a long-running or recurrent illness such as COPD.
Might need to ask an epidemiologist but I would have said a new instance of cancer is as per your examples ,are just new diseases. The fact they have all have an association with smoking is not relevant.
This is a good example of the question being asked for a very particular perspective ,and with a very specific meaning, in this case some related causation. If the patient subsequently developed melanoma, would this be considered to a a ‘secondary primary’?
So, this is a new cancer, but in a person who has already had cancer. “Second time”, or even worse. Not directly related to the first occurrence. This might come from the treatment of the first (or all previous) treatment or genetics or immunodefiency, or just the lifestyle or exposure causing the first cancer not being taken care of. So yes, @ian.mcnicoll a melanoma will be classified as a second primary cancer.
There is a greater risk for cancer in those who already have had cancer, and researchers are working hard to understand why. That’s why it is important to record second primary cancer.
We need to reflect this somehow in our archetypes.
(Apologies for confusing the question by not translate “sekundær primær kreft” properly to English)
An important distinction should be whether the new cancer has origin in the first, i.e. if neoplastic tissue/cells have been left behind (as in local relapse) or spread to a new site (as in metasthasis).
This would definitely be described as a secondary cancer in the UK.
The idea of a 'second(ary) primary cancer seems odd to me, particularly if there is no implied associated aetiology. In the UK this would just be recorded as 2 primary (new) cancers and querying would establish that the person had more than 1 cancer ( via terminology).
I suspect the need for ‘secondary primary cancer’ reflects the original reporting/registry setting i.e it only makes sense if one does not have access to a whole patient past history of diagnoses
Hi! Answering and commenting on @varntzen, @ian.mcnicoll, @heather.leslie and @Anders_Thurin: in Pathology the terminology is indeed often mixed and can be confusing: second and secondary. A second primary cancer I would understand to be exactly as the NCI definition above. But in the same source one reads that “Secondary cancer is a term used to describe cancer that has spread (metastasized) from the place where it first started to another part of the body. Secondary cancers are the same type of cancer as the original (primary) cancer.”
But I’ve always used the term secondary as a cancer or malignancy caused by the treatment, such as:
angiosarcoma after radiotherapy to the breast;
squamous cell carcinoma in an immunecompromised tranplant patient;
a post-trasplant lymphoproliferative disorder (PTLD, which includes all kinds of lymphomas) after eg bone marrow transplant, etc.
In this fashion, if the second presentation of the cancer is related, usually clonally, to a previous cancer, it would need to be further investigated to see if it should be classified as a new primary and not related to a previous cancer. Such a relation would be defined as or explained by:
metastasis = spread by blood vessels, lymphatics, body spaces(colon to liver, colon to lung)
an outgrowth of non-radically excised cancer (eg, melanoma)
regrowth from dormant cancer cells in de bone marrow (eg, after mastectomy for breastcancer)
local relapse (due to genetic field defect, eg in urothelial cancer)
otherwise.
Therefore I try to avoid the term secondary in synchronic or metachronic presentations and hope to be more precise in classifying it, by understanding why a cancer has recurred or is found at another location or after a certain time interval. So this approach differs from the definition of “secondary cancer” in NCI.
If I may use a common language, understandable to me and other not pathologist or oncologist, is it so that we can divide into five groups?
• Brand new case of cancer, never had before
• Recurrence of original cancer - relapse
• Spread of original cancer - metastasis
• Cancer that has arisen as a result of previous treatment, “Subsequently cancer”
• New case of cancer that is unrelated to a previous case of cancer (but might be due to genetics, environmental factors, lifestyle, etc.) “Cancer second time around” (and hopefully not third, fourth)
• Recurrence of original cancer - relapse
• Spread of original cancer - metastasis
These can be pretty blurry in my experience e.g is local spread/recurrence different from metastasis?
I would just say recurrence, then detail what had recurred/spread
• Cancer that has arisen as a result of previous treatment, “Subsequently cancer”
I think that is on a different axis, which is about the aetiology of the cancer = thought to be directly related to the previous cancer.
• New case of cancer that is unrelated to a previous case of cancer (but might be due to genetics, environmental factors, lifestyle, etc.) “Cancer second time around” (and hopefully not third, fourth)
To me this is just a new case of cancer and in an EHR, I would expect the previous cancer to be recorded, so there would be no need to flag that this was second cancer - it would just be there as Cancer #2
@varntzen i would say that both
• Cancer that has arisen as a result of previous treatment, “Subsequently cancer”
• New case of cancer that is unrelated to a previous case of cancer (but might be due to genetics, environmental factors, lifestyle, etc.) “Cancer second time around” (and hopefully not third, fourth)
are both • Brand new case of cancer, never had before
The two are more ralated to why the new primary cancer has accured - and often it can be hard to find out the underlying reason, as it is a multifactoral disease. In my clinical view there is three main categories (with possible undercategories-
new primary (undercateory: subsecuently/adverse event or genetic (or unknown))
recurrence / relapse (undercategory: lokal or metastatic)
progression (growth of already known cancer - either of the primary tumor or metastatic)
Great comments from @ian.mcnicoll and @Ragnhild_Lund_Schult. I like the way Vebjörn @varntzen approached this topic and agree with you all that the blurriness may have to do with mixing time-lines and etiology.
Would it be helpful if I enquire within the Cancer Synoptic Reporting Working Group (CSRWG) at SNOMED International, which I’m a member of, to see if we are able to define these concepts more fully and/or sharply? We meet (live!) in London next week.