Hii everybody!!
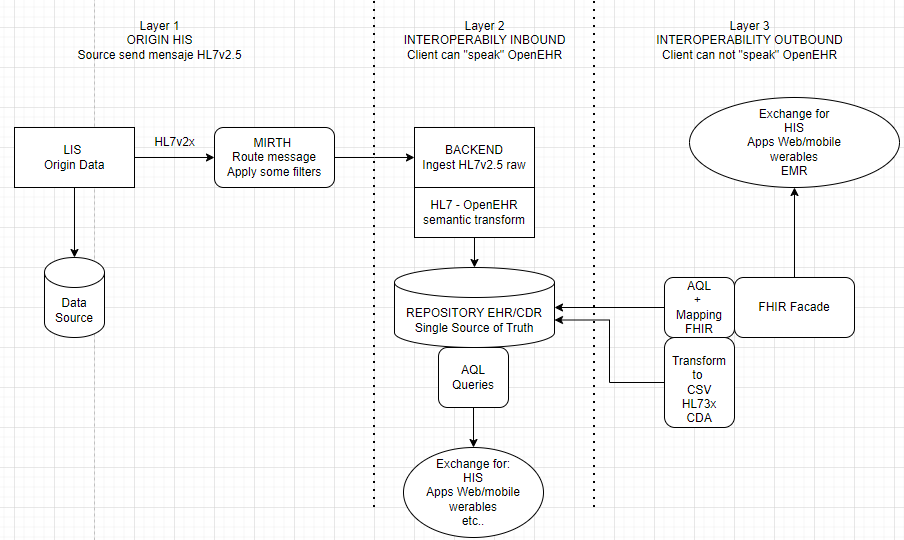
We’re designing a healthcare interoperability platform to integrate legacy Laboratory Information Systems (LIS) with modern Electronic Health Record (EHR) systems and external applications. The goal is to create a semantic-preserving, standards-based architecture that can scale across multiple hospitals.
Current Context:
-
Source Systems: Multiple LIS systems producing HL7 v2.5 messages (ORU^R01, ADT^A08, etc.)
-
Target Consumers: EMR systems, mobile apps, HIE networks, regulatory reporting
-
Requirements:
-
100% clinical semantic preservation
-
Multi-standard interoperability (HL7, FHIR, openEHR)
-
Longitudinal patient records with versioning
-
Scalable architecture for national deployment
Could you help me to improve this dataflow diagram??? Thanx so much!!
That looks about right to me.
You might want to add in a reporting (probably SQL) DB to which you offload reporting and analytics via an ETL process. Native clinical data is tree-shaped and does not play as nicely as you might like with BI tools and population queries. Interestingly, ChatGPT tells me that EPIC does exactly the same - it has an operational datastore based in Cache but a separate RDBMS reporting datastore. AQL makes it fairly easy to populate the ETL, with a little post-processing.
Thank you so much for your time and detailed explanation. I completely agree — clinical data in tree-shaped formats can be tricky for BI and aggregate queries, so having a relational reporting database makes a lot of sense. Using AQL to extract data into an ETL, with a bit of post-processing, seems like a very practical approach.
Best regards!!