Hi, there are two things to consider, what is standard specification and what is technology implementation.
Specification wise, it’s strange that you find anything to do with storage or persistence in the FHIR spec Index - FHIR v4.3.0
Though, in the openEHR spec there is indeed a service layer spec openEHR Platform Service Model and service implementation spec API Overview
The key point of openEHR having such service interface layer is to be able to access the EHR management from external systems.
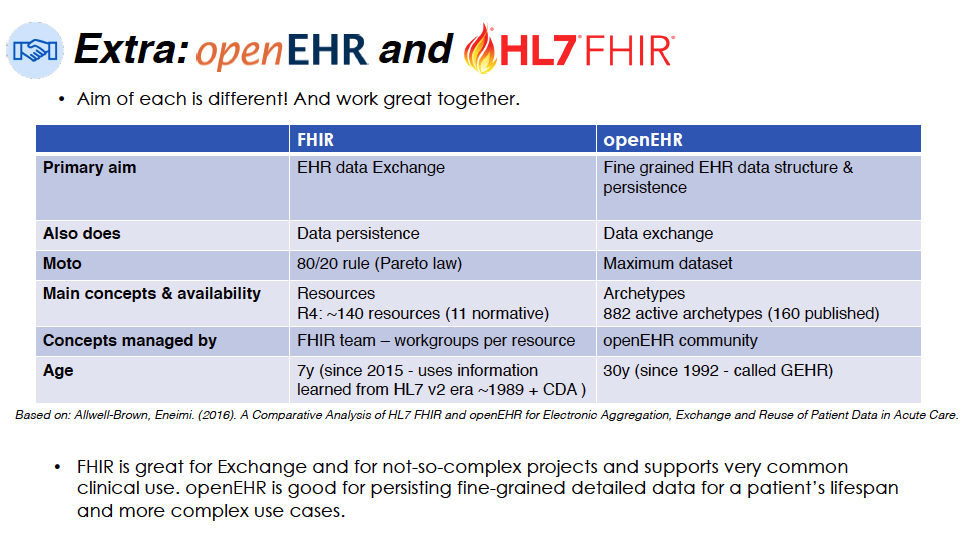
Now, the openEHR scope by the specs is to manage EHR information and provide a data access mechanism that is standardized and based on the same semantic components as the EHR information definition: archetypes and templates. This implies persistence/storage of data.
By the specs FHIR is to operate over data in a standardized REST way (operations, URLs and resources), that is create and retrieve information. This doesn’t imply persistence/storage of data.
Then you have difference technology implementations, based on the specs, but that might extend or go beyond the scope of the standard specs. Like having FHIR storage solutions.
In openEHR the EHR storage solution is the core component of an openEHR architecture, and it is mentioned in the specs Architecture Overview
Even if you have a FHIR storage solution, I would argue the role of such repository is to manage EHRs, while in openEHR that is exactly the role of the storage solution. A FHIR repository can help as a cache, as a secondary analysis database, as a test platform, etc. but it’s not an EHR.
That is why many architectures choose to use an openEHR IMPLEMENTATION TECHNOLOGY PLATFORM to store clinical information, even to access the information using the SERVICE LAYER, and maybe integrate with FHIR by using those openEHR-native services, and use a FHIR IMPLEMENTATION TECHNOLOGY SERVER to receive FHIR requests. I use uppercase here to mark the difference between what is implementation technology and what is standardized in the specifications, so the main thing is: implementation technology can go beyond what is strictly specified in the specs.
So don’t be confused, spec is one thing and technology is another thing.