Hi Simon,
Welcome to the community. You’ve not started with an easy task.
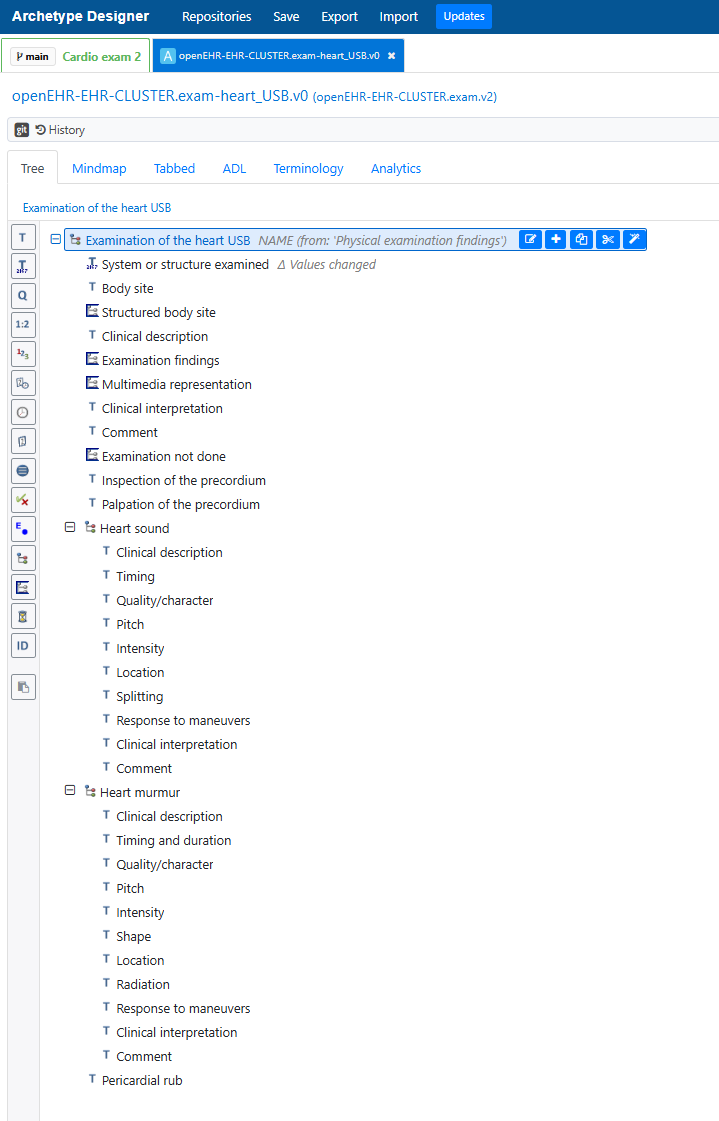
Yes, the pattern is still the basis for creating physical exam archetypes.
I would start as simple as you can, especially if this is a new experience for you. Also to keep it aligned with what current systems are recording, knowing that we can grown it and extend it in the future.
More specifically, I would advise you to begin with investing time in developing a mind map outlining your proposed pattern, including links to related archetypes. This is a way of testing whether the pattern will work before you commit to building an archetypes Just adding the data elements that you know you need and are pretty sure will be ubiquitous. While we are aiming for inclusivity of all information about the heart it doesn’t all have to happen at once. That said, the mind map will help identify the road map for other possible data elements or related archetypes as well - effectively an ecosystem of the heart/chest related archetypes.
Only once the mind map is agreed by your peers, would I start to use the Archetype Designer tool. This advice is one of the best kept secrets, in terms of not wasting time. Mind mapping is a much more effective tool to test a modelling pattern.
The oedema archetype originally designed to be nested in any higher level Exam CLUSTER, for example, the theory was to nest it in an archetype related to the lower leg, to record pitting oedema of the calf. But again, looking at this very old archetype, it also needs some more work to make this clearer. OR We need someone to do the investigation (via mind mapping) to work out if it is more efficient to just add relevant data elements in the ankle/leg/sacrum archetypes and if there are other use cases for oedema that would make this archetype inappropriate.
Cyanosis may be best modelled directly and explicitly in the Exam archetypes where cyanosis is examined eg face, fingers or create a reusable one for broader reuse. Again, we need further modelling and investigation before we can make that decision.
There are some heart-related archetypes that have been rejected (and the underlying reason for Ian’s PTSD) and the ‘Auscultation’ CLUSTER that @ian.mcnicoll pointed you to has some good possible content related to heart sounds even though the concept is not correct. Heart sounds could be modelled as an internal grouping/cluster in the Exam of the heart archetype, although I wonder if there is ever a use case where we might record heart sounds outside of a formal heart examination? For example, if there is a rupture of the diaphragm, you can hear breath sounds in the abdomen. Is it also possible to need to record heart sounds within an ‘Exam of the abdomen’ archetype context?
I have certainly used my dusty old version of Macleod to assist in designing these archetypes, but I’d also just caution you to remember that we are not designing them for academic purity but to reflect actually clinical practice, which may be somewhat messy and we need to be able to capture recording for the least untrained or remote health workers who may only be able to document that a murmur is present, through to the most experienced cardiologists who want to document every diagnostic ‘click’.
This is our ‘art’ and calling in designing high quality archetypes and, simultaneously, our collective world of pain! You are not alone, it is challenging but also very satisfying when you ‘nail’ an archetype and it gets published.