Here we are talking of different scopes. There is a difference between modeling a problem and modeling a problem list, and that’s what I tried to ask in my original question. The fact of having a diagnosis could (should?) be documented per se, independently of being later incorporated to a summary list.
This approach also provides much more flexibility, since you can build multiple list: a complete list of problems, a list for just open problems, lists for primary care/specialized care problems… And for each list we could use different templates for the problem/diagnosis.
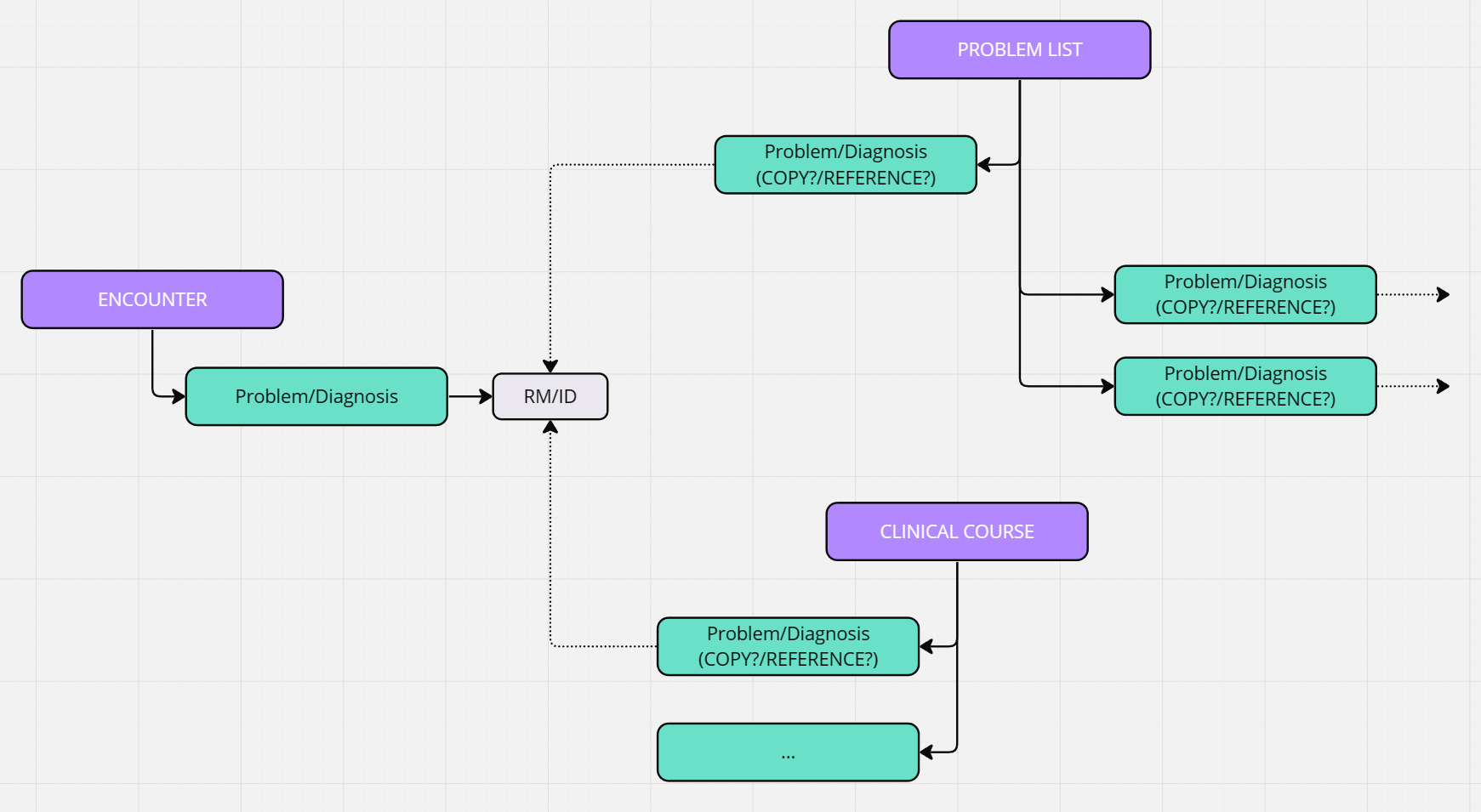
There are well known problems about building those lists, including:
- Is the information copied/duplicated of just referenced from the list to the original composition? More about this in How accurately do we model "copied" data?
- Is the list manually maintained and curated or the result of an on-the-fly query?
- Are the systems able to deal with those queries efficiently? Are we even able to express them?
Finally, having the problems originally recorded in the list might not be an error depending on the circumstances, but I think you will lose many contextual information.