Hi!
We have a clinical use case where medications for pediatrics are going to be prepared by using different medicinal products.
As you all might know, medications for pediatrics are highly dependent on weight. Therefore, nurses need to use medicinal products and prepare their required medicine by combining different products and having precise doses for patients.
one example is: vancomycin 5 mg/ml solution for infusion diluted in glucose 5%
There is no pre-prepared dose for this medication so the nurse should prepare it in the point of care.
We need to use SNOMED CT codes for data entry. What is the best way to capture the final medication in the information model?
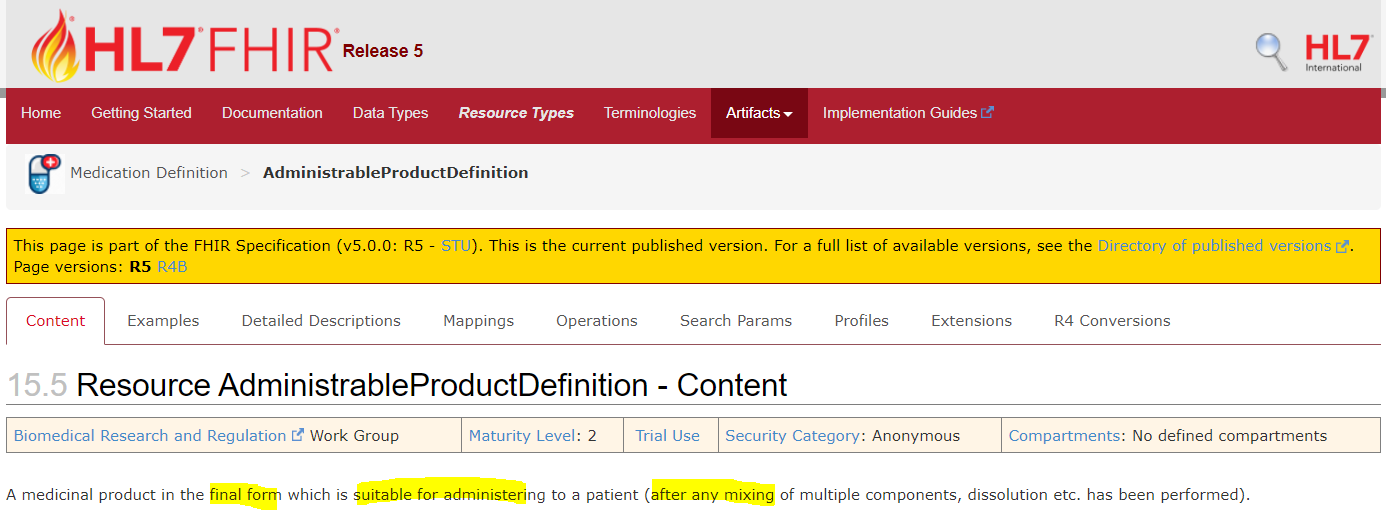
The final medication should be an intermediate result of executing the medication order, and would be used in the subsequent process of administration. This is my current understanding. Am I right?
This is a pretty complex area but I think in the UK, this work would normally be done by the hospital pharmacist, and would be regarded as part of dispensing.
As such, my first thought is that this might be best carried in an ACTION.medication archetype with a ‘Medication prepared’ careflow step set. (See the pathway tab in CKM)
You could set up a specific Chemo preparation template which would include this Ation archetype alongside height and weight archetypes and any other background data needed.
You could definitely use SNIMED CT for some parts of the model but not others. Where the data points are already ‘named’ in openEHR, you can always capture any matching SNOMED CT terms using term mappings. If you need help with that, I suggest you star an other topic and give an example .
@ian.mcnicoll You are right. we have some information from UK which shows that they were building a hierachy for virtual medicine in their SNOMED CT extesion just because they wanted to capture all different medicines that are not realy exist. NHSDigital SNOMED CT Browser
You can definitely use SNOMED-CT as part of drug naming/coding but essentially dm+d is the of truth but is then tagged with SCOMED codes. There is something very similar in Australia - AMT.
In general, here (zh-cn), the preparation of fluids for infusion ([quote=“MaryamRazavi, post:1, topic:5766”]the final medication[/quote]) is a nurse’s daily routine.
In CN, the preparation of chemotherapy drugs is also part of the daily work of nurses, although the nurses who perform the preparation operations need to be specially trained.
@ian.mcnicoll All dm+d have created under virtual medicine hierarchy i UK SNOMED extension. That means there is SCT code for dm+d. Can you please explain little bit more about “tagged by SNOMED code”.
@linforest same here. Are you using SNOMED codes for capturing the final product that nurses preparing? Or other word can you please explain how you are capturing the data when it is coming to this specific use case?
Just that dm+d is managed a seperate entity and then SNOMED terms are added for the product and substance names plus routes of administration but not everything in DM+d is built from SNOMED
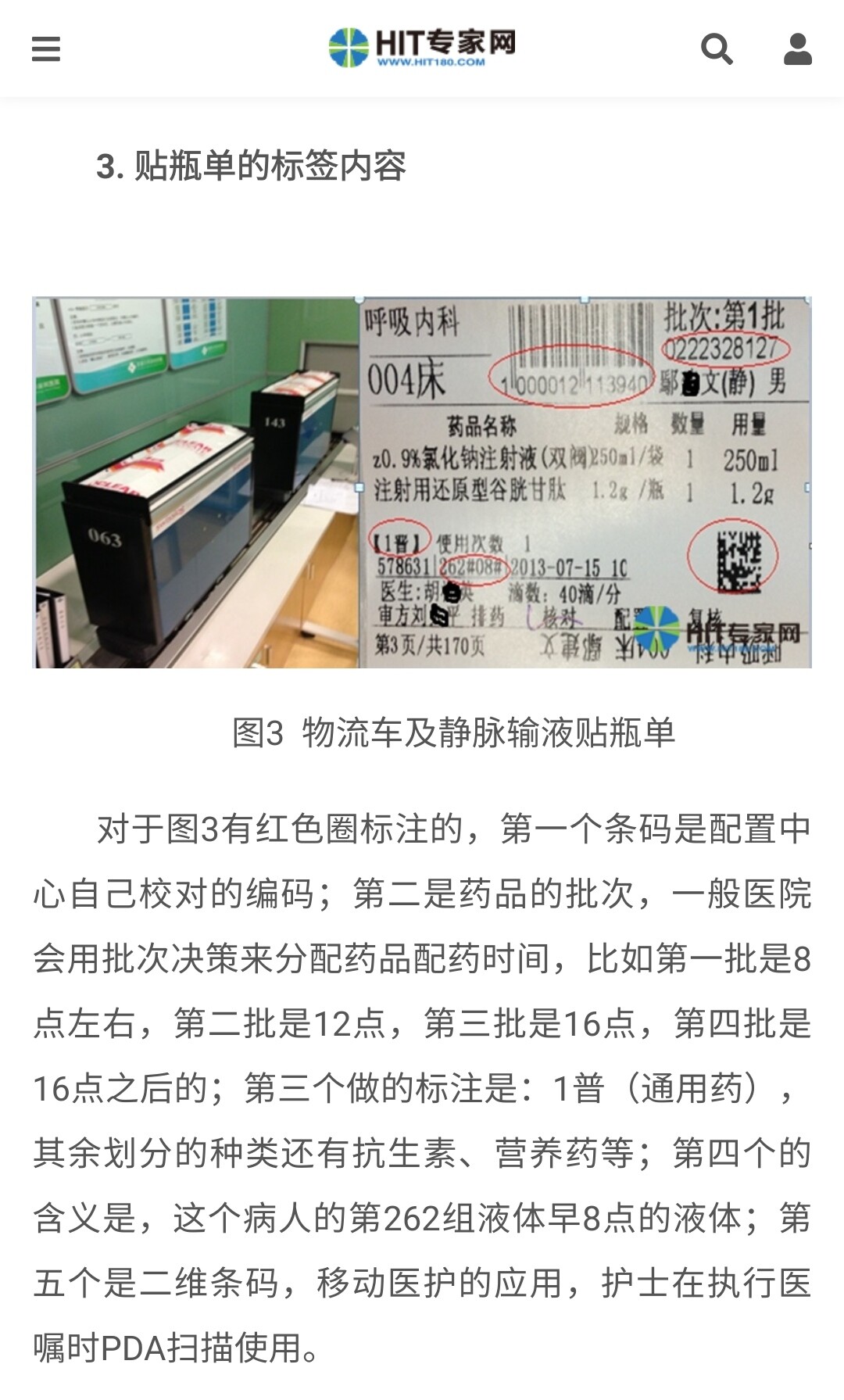
Our national Ministry of Health has made general regulations on the labelling of final infusion preparations. And the part you are interested in is the information on the medication order. In practice, the list of dosages and specifications of the constituent medications is often indicated on the label.
The following are the guidelines for the construction and management of intravenous medication dispensing centers issued by the Ministry of Health (for trial implementation):
Sorry, I have little knowledge/experience on pharmacy stuff. On the example label above, the barcode on the top is a pack entity id assigned by the dispensing center and it should be associated with the relevant medication order. There is a category of the final preparation (example value here: ‘1 普’ for general medication; other values including antibiotics, nutrition…) but no concept code/name for the final preparation.
I understand the design. One thing is just kind of a question for me. What is the purpose od SNOMED codes in this case. As much as I know, we try to use SNOMED codes for interoperability and also generating analytics report for reseach. As I understood the SNOMED codes in the UK have extra attributes which are not supported by MRCM (Machine Readable Concept Model) therefore Expression Constraint Language (ECL) which is a qury language on SNOMED is not applicable.
Can you give us one example about one use case? How you are thinking to use SNOMED codes in the model? OR if you want I can take a clinical use case to discuss it here?