That sounds great, thank you!
And no worries about ophthalmic knowledge, i guess technical expertise is much more important for now. I like to think that I have reasonably good overview of VA testing from the clinical side.
Plus I have a bit of a collection of (fictional but realistic) VA testing scenarios of varying complexity from very kind colleagues in different countries, which which can be helpful to check which in which models they do or do not “fit”.
thank you for offering to set up a zoom call, i think that’s a good idea. I’m in Germany so GMT+1 but generally flexible.
You will also see that the 'Visual acuity test result archetype has been undergoing a review, but this appears to have stalled way back in 2013 with a second review round unresolved.
Remember that the FHIR profile will be based on the underlying Observation FHIR resource and that adds additional content that may not be required for the visual acuity use case, whereas the archetype will possibly be much leaner and utilise the underlying openEHR reference model attributes as necessary. That said, we would welcome alignment where possible.
I’d like to volunteer @varntzen as CKA lead, at least to coordinate efforts so that we can bring it back to the community via CKM, and possibly myself if we can manage time zones - I’m in Melbourne, AU which unfortunately adds an extra layer of complexity in coordinating meeting times.
@ian.mcnicoll initiated the last review round and may recall why the review was abandoned.
TBH I can’t really recall why the original Visual Acuity review stalled. I don’t recall that there was any particular major issue raised, just lack of time/ resource I think
It was very much based on input from specialists at Moorfields Eye Hospital, particularly Bill Aylward who originated openEyes.
I did get a little bit of feedback from on e of e openEyes developers who said that the archetype did not play as nicely as he had hoped in terms of visual acuity testing workflow e.g Pinhole testing then with visual aids, without aids etc, so that might be worth looking at again.
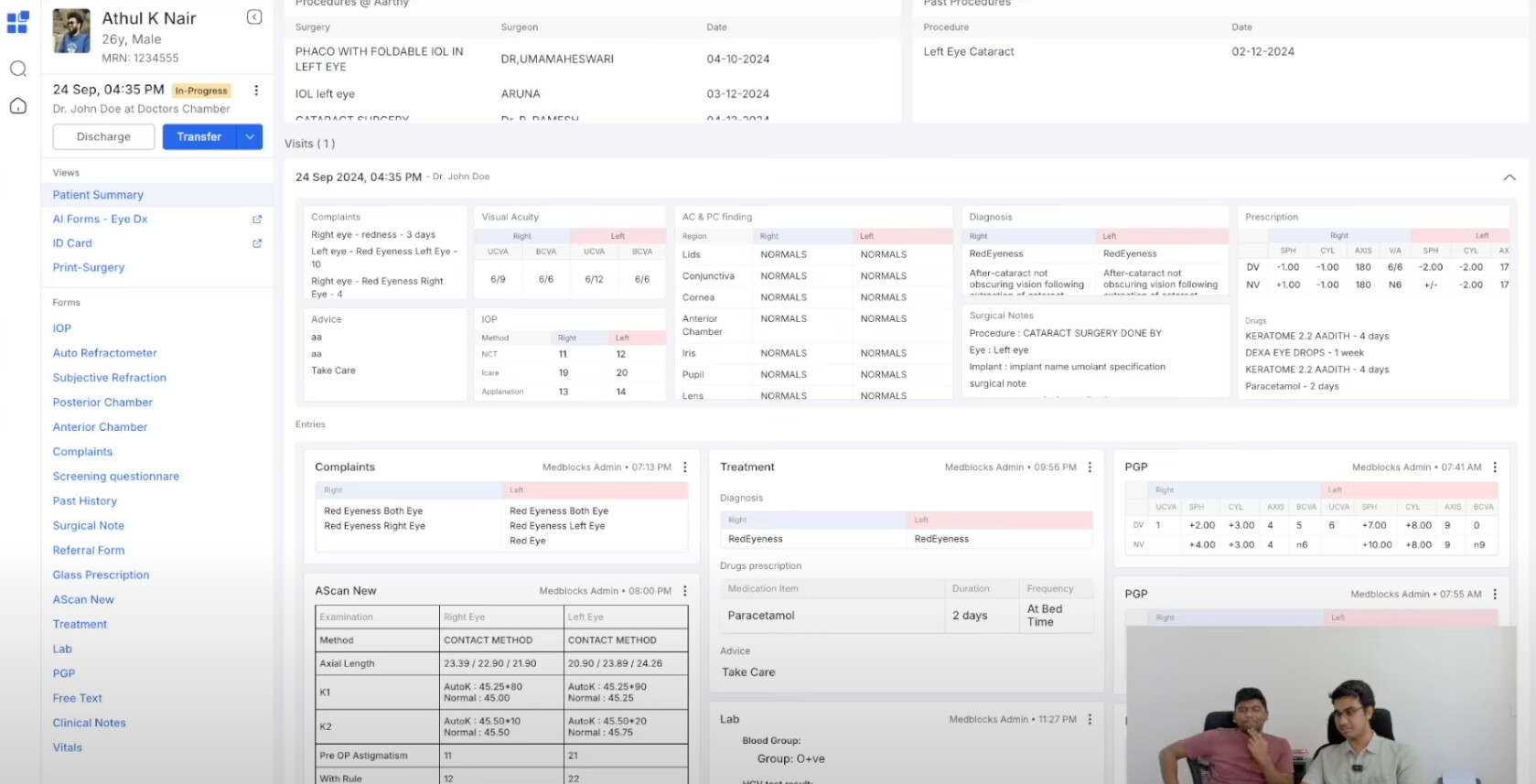
I just watched a wee MedBlocks demo of an opthalmology solution they are developing
@Sidharth_Ramesh - how has the visual acuity archetype worked for you?
My only advice would be to really keep the scope tight - Optom is highly specialised - stick to some common pathways - glaucoma, cataract to start with.
Hey @ian.mcnicoll, yes, I can help provide the data models.
@poorna can we provide a dump of all the archetypes and templates we’re using?
I know a lot of them aren’t modeled perfectly, but at least we start a conversation around this.
Thanks for pointing me to the Ophthalmology Project in the CKM, i will dive into the other Archetypes when I can .
And many thanks for volunteering as CKA lead for the VA archetype!
I already have ideas for things we could try and improve, i will write them down for discussion.
In terms of time zones late evening or early morning German time would be OK for me, too at least to get things going.
I have read through the Contrast sentitivity Archetype proposal from @Olha_Nikolaieva and offered my comments, we’ll try and work together on this.
But i do think it makes sense to consider the relationship between the Contrast Sensitivity and Visual Acuity Archetypes, as they are the two sides of the same coin do some degree. (there has to be contrast to resolve objects, and there have to be resolveable objects to measure contrast sensitivity).
I think it would be very helpful for the CS Archetype if we improve the the VA Archetype first, because:
Lots of Items in the contrast sensitivity Archetype can be taken from the VA Archetype (Which eye, distance, Correction etc.), some of these require changes (for example the SNOMED-Codes For entire Right/Left Eye are inactive. Right/Left eye region may be better.), potentially the correction as well
The contrast sensitivity archetype proposal currently contains some methods which are actually “low contrast” Visual acuity tests (symbols get smaller and smaller under low contrast conditions). If we manage to model the contrast inside the Visual Acuity test ressource then these are actually more appropriate there.
So i think it will be much easier to build the contrast Sensitivity Archetype based on an improved VA Archetype, and i hope we can do both.
Please let me know if you have anything specific that I should look at or do to prepare.
Hopefully today’s course by @Sidharth_Ramesh will help me get me up to speed
I think it very hard not to underestimate the complexity of even something as central to ophthalmology as Visual acuity Testing.
VA testing is highly modular in real life as we are pretty free to combine things we put in front of patient’s eyes (such as own glasses PLUS pinhole or contact lens PLUS trial Lenses)
In FHIR this made me allow any number of component slices to specify a correction in front of a specified eye, such as contact lens plus trial lenses here
This could also be done for own Glasses or trial lenses PLUS pinhole, which is not that uncommon clinically, we do this to find out whether there is a component of irregular Astigmatism as it occurs in diseases like Keratokonus.
So If we want to stay close to clinical reality specifying multiple type of corrections in front of each eye should be possible.
I am extremely happy to see that @Sidharth_Ramesh and @poorna are working in Ophthalmology, that really is a great thing to happen to our field!
Building a User-Friendly UI for highly granular data models in Ophthalmology is extremely challenging, but I’m hopefull that this will not scare you off and I’m happy to help if you want me to!
Regarding the Scope:
I agree about keeping it tight, think even pathway like cataract may be too large of a scope initially if we thing about everything that a patient getting cataract surgery goes through.
I think it makes sense to focus on the very central, very basic clinical observations that are shared by pretty much all clinical pathways (such as VA testing), as the Ophthalmology Project in the CKM has done, and tackle these one by one before trying to model an entire pathway.
There is an existing Ophthalmology collaboration incubator in the CKM, https://ckm.openehr.org/ckm/incubators/1013.30.95, dated back from 2021. It’s empty by now. I suggest we use this incubator to upload archetypes that already exists locally. Some of them will eventually be moved to the Ophthalmology domain project . The incubator is per now private, which means users have to be named as Editor or Reviewer in order to enter. (Reviewer is misleading, it’s not possible to run reviews from an incubator).
I would like to invite you to a kick-off online meeting to discuss how we can pick back up on ophthalmic archetype development.
I would suggest an initial focus on the Visual Acuity Archetype, because its review has been suspended since 2013 and it would absolutely be worth figuring out how openEHR and FHIR data models could align for this central observation.
I would be very grateful if you could indicate your availabiliy if you are interested:
To begin with here is the list of defined structures in Finland. The Finnish name has link to our code server with info in Swedish (except the ortoptic form)– in case it doesn’t open, I can pick the detailed documents. Are any of these on level of achitype or are they all templates, is a good question.
Something that I wanted to add because it should not be overlooked:
Aitor Eguzkitza has done a tremendous amount of modelling work in this incubator approximately between the years 2014-2016 while at the universtity of Navarra.
I will need to spend more time looking through this incubator to comprehend models, but I think we should take them into consideration going foward!
And I’ll try and reach out to him..
I wanted to let you know we’re preparing a review round for therevised draft of the intraocular pressure archetype. This means if you have eye care professionals in your network it might be a great time to reach out to them. If you connect them with me to I will try and get them interested in becoming a reviewer (Bonus points if they work in countries other than Germany and the UK) .
I like to think that we have gathered a little bit of momentum, in large part due to the unwavering patience of @heather.leslie@ian.mcnicoll and @siljelb , even during long discussions on the semi-quantitative evaluation of the squishiness (or non-squishiness!) of eyes on palpation.
I also want to note that we have not given up on the visual acuity Archetype, but decided it may be best to first gather experience reviewing an Archetype that is a little bit simpler. A long-term record of IOP data is extremely important for glaucoma care, so this was an obvious choice
Many thanks to everyone who has helped this effort so far, especially to:
The three mentioned above plus @arielyho for their help with our Introduction to openEHR written specifically for eye care professionals in mind.
To Ian Rodrigues from the openEyes team for lending his expertise as a glaucoma consultant to the revision process.
Please to get in touch if you are interested in doing anything with openEHR in the eye care domain in the future - especially if the Archetypes are not quite there yet for your use case. Our meeting times are on the landing page, feel free to drop in.
The deadline will be the 11th of January due to the holiday season, and because we are still working to invite more first time reviewers from the eye care professions.
If you want to participate as a reviewer or know somebody know might be interested please don’t hesitate to get in touch.
We have completed the first review round of the Intraocular Pressure Archetype.
With 21 reviewers from 9 different countries participating we got 6 votes to ‘Accept’ and 15 votes for ‘Minor Revision’. [1]
I am exited to report that 15 eye care professionals lend their time and knowledge to this process, among which were experienced glaucoma experts.
For 17 of the reviewers this was the first CKM review of their life, so congratulations and many thanks to them!
Even though we did not get any votes for a ‘Major revision’ we still made some significant changes based on the >100 comments we got from reviewers. So we angreed to have a second round, which is currently live. Please do get in touch if you want to participate!
Many thanks to @Pete_Bouvier for his help in designing a little logo for our open working group, which I think will be super-helpful as we try to engage colleagues to participate in our Archetype modelling efforts:
Out open working group still usually meets at the last Thursday of the month at 12:00 CET (except next week’s meeting will likely be rescheduled to the 5th of March). Feel free to say hello there!
Many thanks to everyone involved, especially to @ian.mcnicoll, @heather.leslie and @siljelb , their guidance & unparralleled patience with us eye care professionals is absolutely essential to this effort!
More precisely they were 25 reviewers due to an extra review round in Norway facilitated by @siljelb . ↩︎