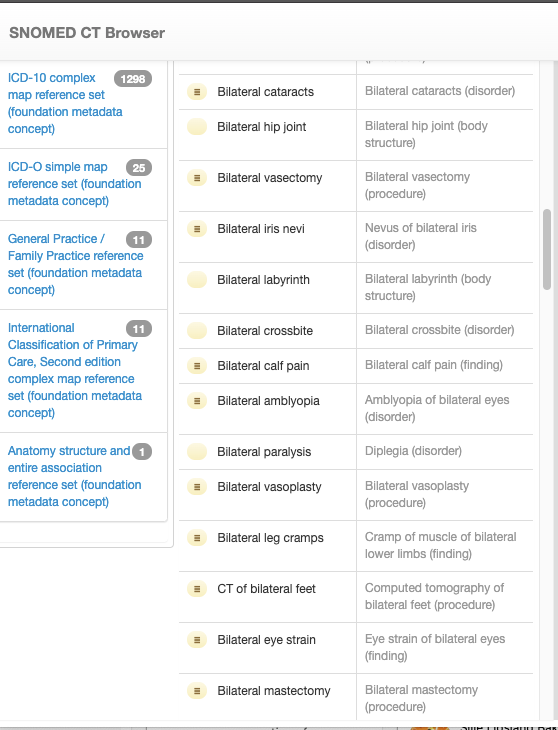
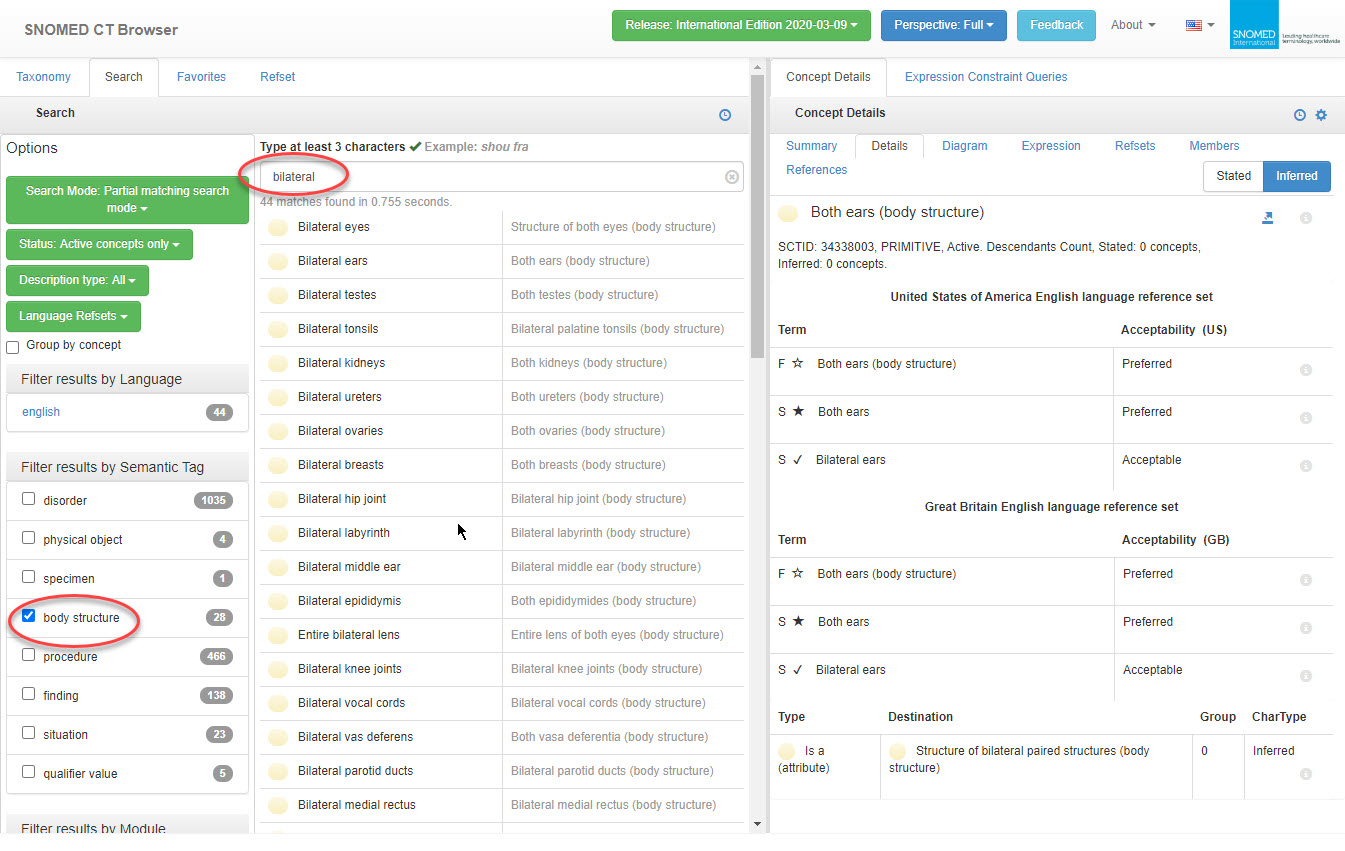
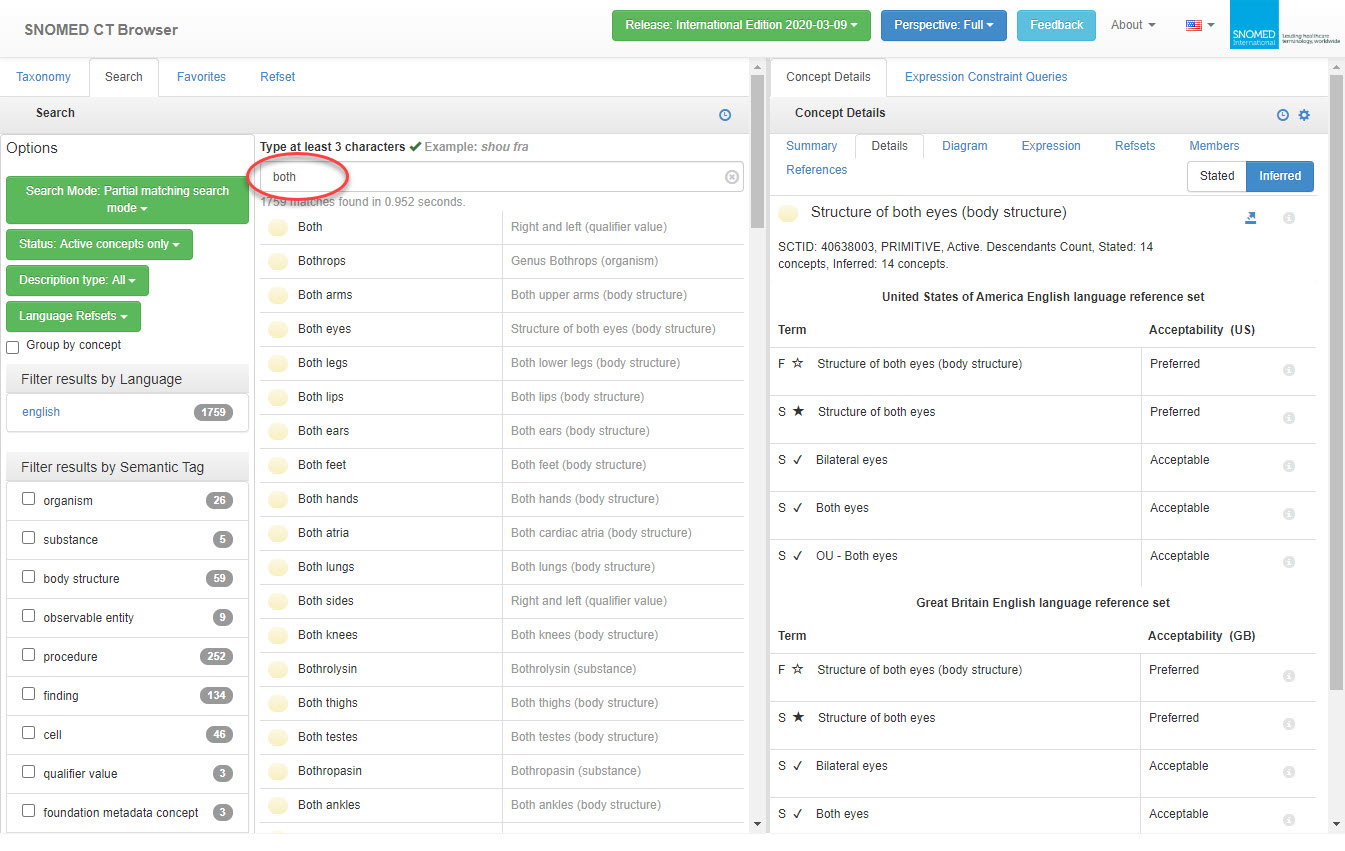
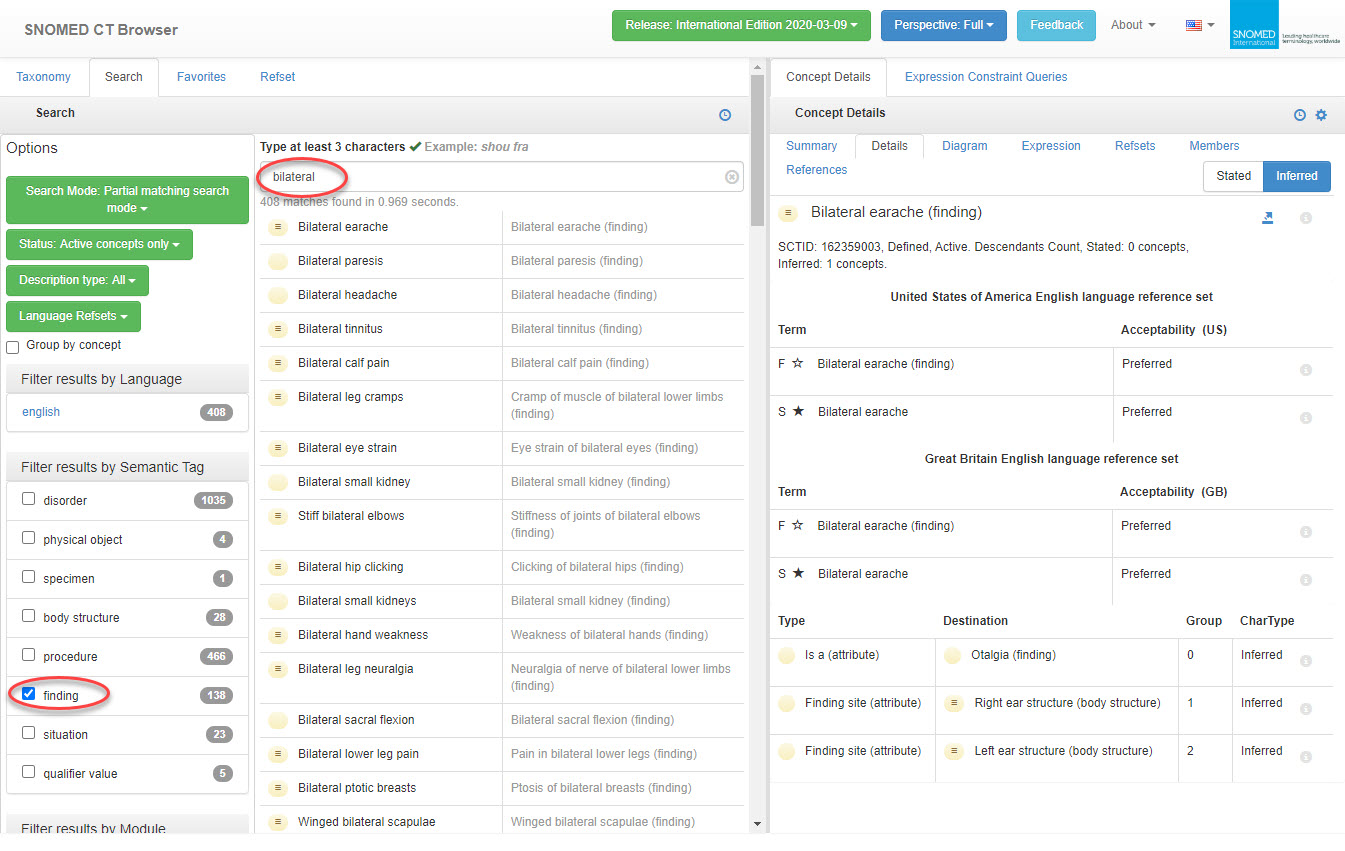
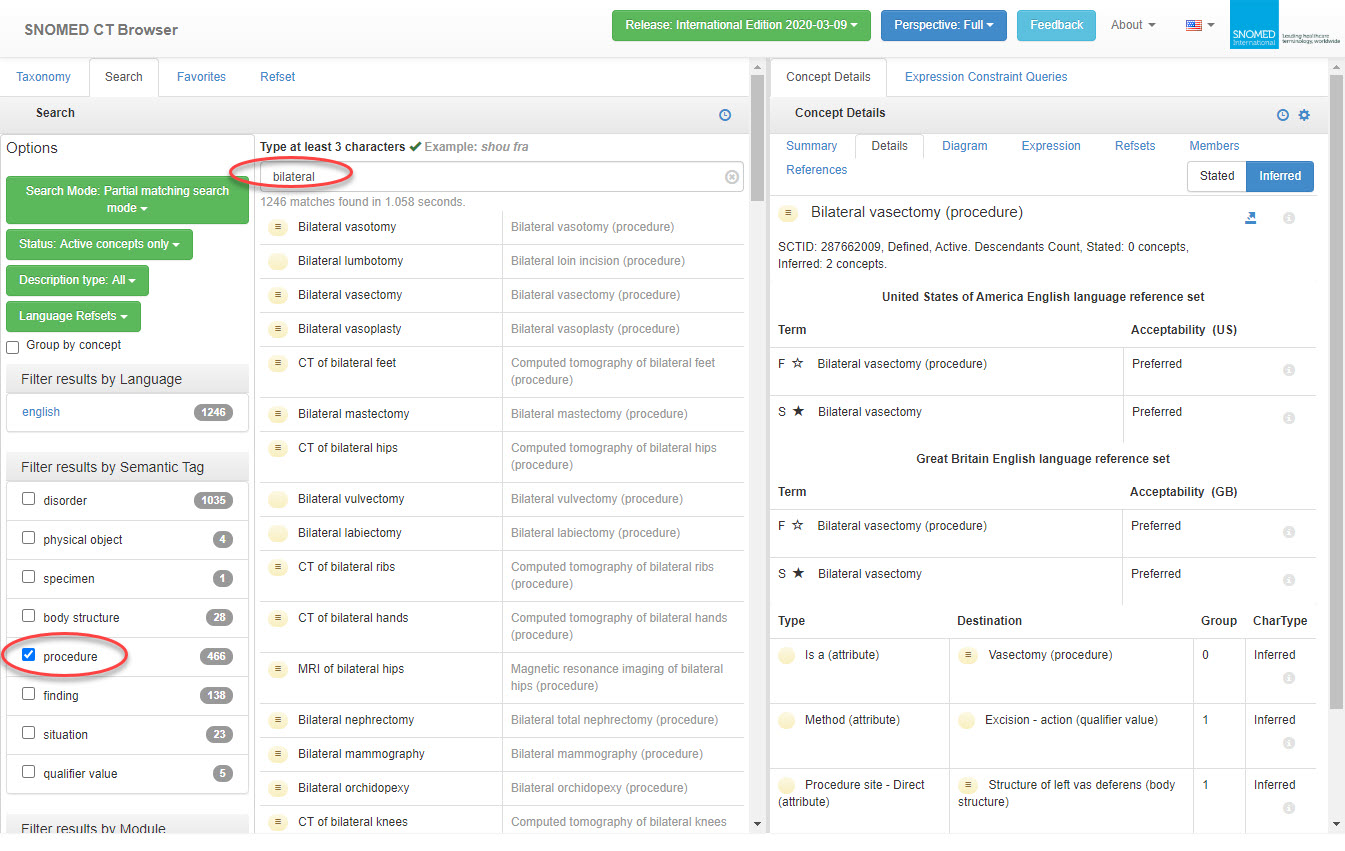
Looking at the SNOMED example you provided - structures usually are recorded as both in the preferred/FSN, although bilateral is often available as a synonym. I certainly don’t usually talk or record body sites as bilateral ears or bilateral hips, rather both ears or hips. ‘Both palatine tonsils’ is not an option, only ‘bilateral palatine tonsils’ but I’d suggest that’s a SNOMED issue and an outlier - at least it is plural! ‘Bilateral middle ear’, singular, makes less sense.
Recording ‘Bilateral pneumonia’ is different to recording ‘Pneumonia’ in the left and right lungs. Currently the Problem/Diagnosis archetype allows recording of:
- Diagnosis name = “Pneumonia” | Body site (0…*) = left lung ( SCTID: 44029006) +/- right lung ( SCTID: 3341006)
- Diagnosis name = “Pneumonia” | Body site (0…*) = both lungs ( SCTID: 74101002)
- Diagnosis name = “Pneumonia” | Structured body site SLOT/CLUSTER.anatomical_location (0…*) - Body site name = Lung | Laterality = left or right
- Diagnosis name = “Pneumonia” | Structured body site SLOT/CLUSTER.anatomical_location (0…*) - Body site name = Lung | Specific site = Base of right lung ( SCTID: 51785002) Laterality = left ( SCTID: 7771000) or right ( SCTID: 24028007)
- Diagnosis name = “Pneumonia” | Structured body site SLOT/CLUSTER.anatomical_location (0…*) - Body site name = Lung | Specific site = Base of lung ( SCTID: 10024003) Laterality = left or right
So we can record Pneumonia found in the left lung, right lung (#1) or both lungs (per #2), but we don’t record pneumonia in ‘bilateral lungs’ at least not in common parlance. But adding ‘bilateral’ or ‘both’ to the ‘Laterality’ data element in anatomical location is not actually helping you record ‘Bilateral pneumonia’ as an entity.
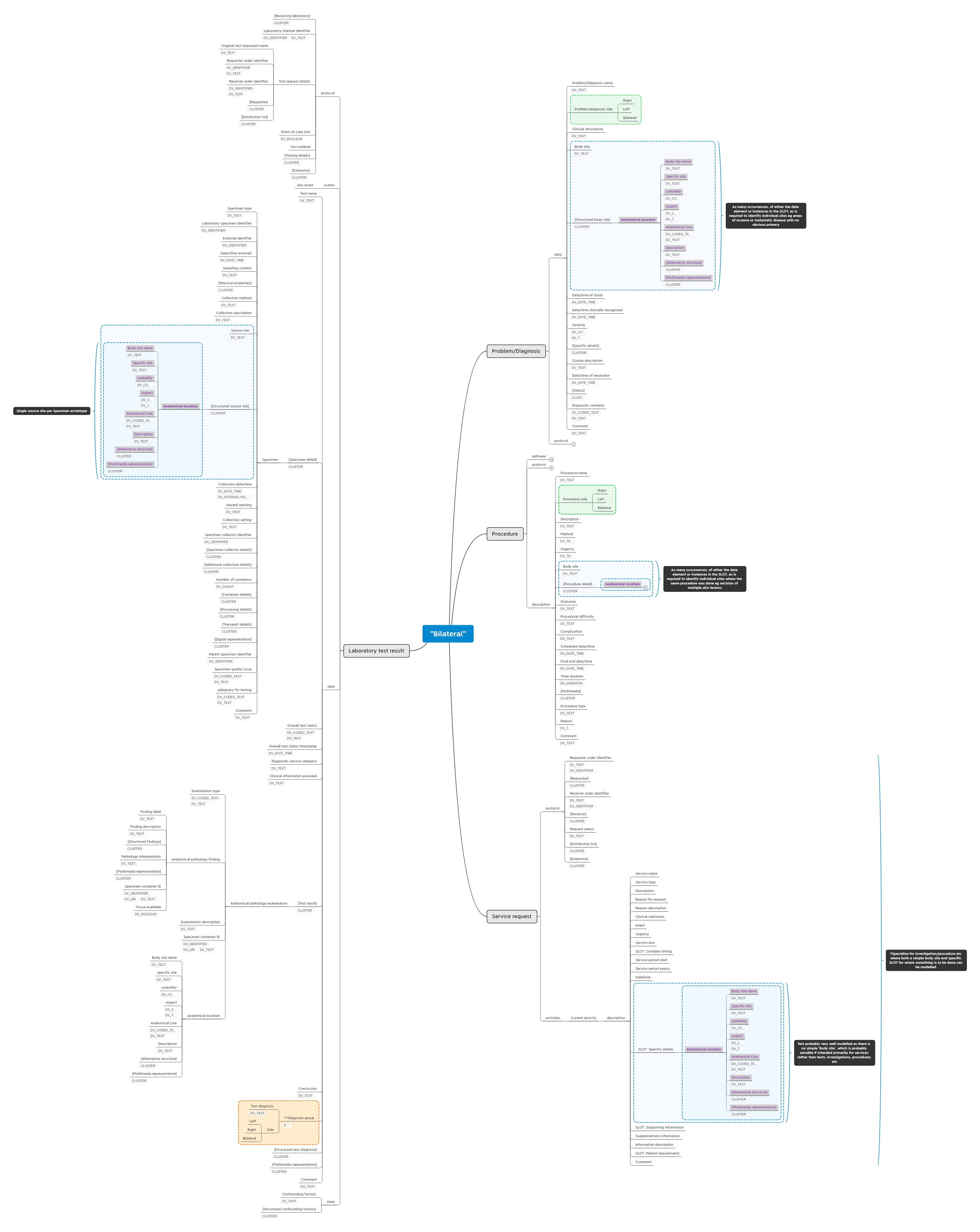
I propose we should a qualifier of ‘Side’ for the Problem/Diagnosis name in the Problem/diagnosis archetype with the values Left/Right/Bilateral, if it is not available as a pre-coordinated diagnosis term (see green box in mind map, below). And CLUSTER.anatomical_location remains unchanged as a the way to record details about a single body site.
I think it is the same in principal for Procedure (see mind map) - I propose we should a qualifier of ‘Side’ for the Procedure name in the Procedure archetype with the values Left/Right/Bilateral, if it is not available as a pre-coordinated procedure term
Re Service request - at present we don’t really have any way of addressing a side eg to order bilateral mammography if this is not already available as a pre-coordinated term. We do have SCTID: 43204002 for Bilateral mammography, so not a good example, but we need a way to represent those that aren’t pre-coordinated. We could do the same thing, but it makes little sense to see Side and Body site in a Service request in the broadest sense, but perhaps makes more sense if we specialise it for Procedures/Investigations etc and add Side and Body site to align with my proposal for ACTION.procedure.
CLUSTER.specimen correctly carries one anatomical site per specimen, so needs no further modification.
Lab findings (eg in CLUSTER Anatomical pathology) will be related to the specimen, so not likely requiring left/right/bilateral/both.
Imaging findings may need left/right/bilateral. Although I suspect each finding should be recorded and described individually eg multiple lesions of different shape/size/location.
Lab and Imaging diagnosis will be similar to Diagnosis. However there may be multiple findings, so the we may need to look at creating an internal cluster ‘diagnosis group’ to handle the Left/right/bilateral qualifer per lab/imaging diagnosis (see orange box in mind map)
2020 06 04 Bilateral_Anatomical location.xmind (212.3 KB)
Thoughts?